
Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(3); 2023 > Article
-
Case Report
Penetrating gallbladder injury in a pediatric patient: a case report -
Nelimar Cruz-Centeno, MD
 , Shai Stewart, MBBS, Derek R. Marlor, MD, Charlene Dekonenko, MD, Richard J. Hendrickson, MD
, Shai Stewart, MBBS, Derek R. Marlor, MD, Charlene Dekonenko, MD, Richard J. Hendrickson, MD -
Journal of Trauma and Injury 2023;36(3):295-297.
DOI: https://doi.org/10.20408/jti.2023.0008
Published online: July 5, 2023
- 696 Views
- 21 Download
Department of Pediatric Surgery, Children’s Mercy Hospital, Kansas City, MO, USA
- Correspondence to Mailing Address: Richard J. Hendrickson, MD Department of Pediatric Surgery, Children’s Mercy Hospital, 2401 Gillham Rd, Kansas City, MO 64108, USA Tel: +1-816-983-6335 Email: rjhendrickson@cmh.edu
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Penetrating gallbladder injuries are uncommon in the pediatric population. The treatment varies according to the severity of the injury and the patient’s hemodynamics. We present the case of an 11-year-old male with an accidental pellet gunshot wound to the right upper abdomen that resulted in a grade III liver laceration and damage to the anterior gallbladder wall. The patient underwent laparoscopic cholecystectomy with drain placement. Postoperative radiography of the surgical specimen confirmed the presence of the pellet in the gallbladder. The patient recovered uneventfully and was discharged home on postoperative day 3. Laparoscopic cholecystectomy is a feasible treatment option for penetrating gallbladder injuries in hemodynamically stable patients.
- Traumatic gallbladder injury is uncommon, accounting for 1.9% to 2.1% of all cases of abdominal trauma [1]. In the pediatric population, these injuries are more common with blunt trauma and are associated with liver lacerations in approximately 83% to 91% of cases [1]. Moreover, the occurrence of a gallbladder injury in a pediatric patient secondary to penetrating abdominal trauma is a rare event. An extensive literature search revealed only one reported case of a penetrating gallbladder injury in a pediatric patient that occurred more than five decades ago [2]. The case was managed with open abdominal exploration and primary repair of the gallbladder wall defect. This highlights the infrequency of these cases and the importance of describing current and more up-to-date management options and their subsequent outcomes.
INTRODUCTION
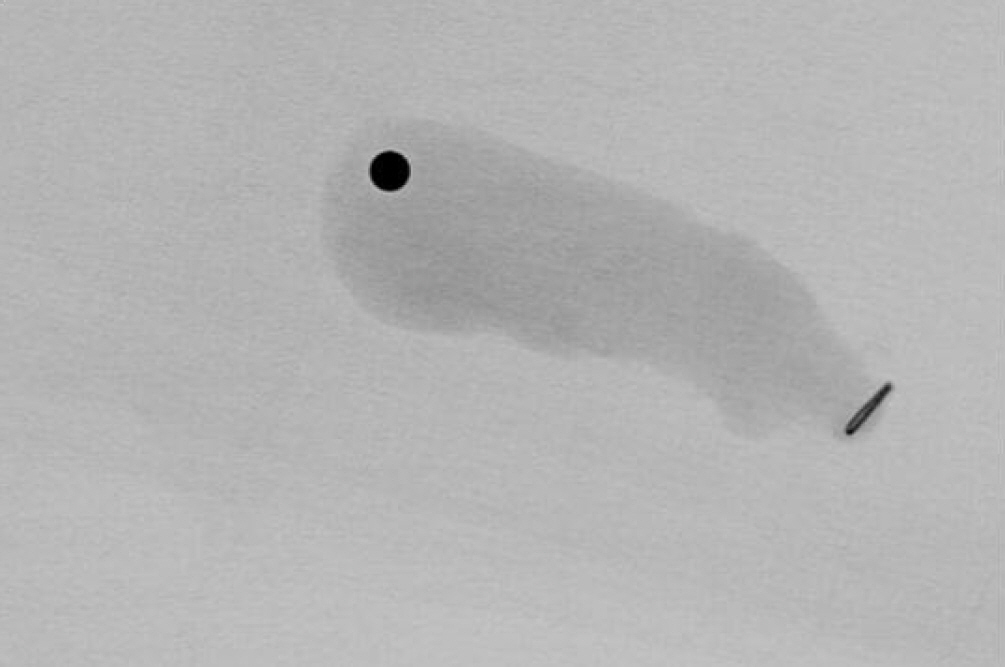
- We present the case of a healthy 11-year-old male patient who sustained an accidental gunshot wound to the right upper abdomen with a pellet gun. The patient was taken to a peripheral hospital where basic laboratory and imaging studies (chest and abdominal x-ray examinations, and chest and abdominopelvic computed tomography scans with intravenous contrast) were performed before he was transferred to Children’s Mercy Hospital (Kansas City, MO, USA). The patient was hemodynamically normal and laboratory investigations were remarkable for reactive leukocytosis of 17.7×109/L and mild transaminitis with alanine transaminase and aspartate aminotransferase levels of 52 and 61 U/L, respectively. The bullet traveled through the right seventh intercostal space, resulting in a grade III liver laceration measuring 3.8 cm in length and extending from the anterior surface of the liver to the gallbladder fossa, with a small metallic object adjacent to the gallbladder fundus, pericholecystic fluid, and mild thickening along the colonic hepatic flexure (Fig. 1). Upon arrival at our institution, the patient remained hemodynamically normal. The physical examination was remarkable for a 2-mm penetrating wound in the right upper abdomen associated with tenderness to palpation with no peritoneal signs. Given the patient’s penetrating abdominal injury with associated abdominal pain and suspicion of intestinal injury, the decision was made to perform diagnostic laparoscopy. Upon entry to the abdomen and inspection of the bowel with close attention to the colonic hepatic flexure, no intestinal perforation was identified. However, there was bile spillage and blood at the right upper quadrant, as well as damage to the anterior gallbladder wall. On the anterior liver surface, a small wound from the bullet was visualized with no active bleeding. An intraoperative x-ray examination was used to localize the pellet, which was observed to be in the gallbladder. The decision was made to perform laparoscopic cholecystectomy. After the gallbladder was removed, an additional small wound was seen at the gallbladder fossa, most likely from the bullet trajectory causing the liver laceration, which was mostly intraparenchymal. No bleeding or bile leak was observed, and no additional interventions were required. An x-ray of the surgical specimen confirmed the presence of the metallic pellet inside the gallbladder lumen (Fig. 2). A drain was left in the gallbladder fossa due to the high-grade liver laceration. During the postoperative period, the patient tolerated a regular diet and pain was minimal. Once the serosanguineous drain output decreased to a satisfactory volume, it was removed on postoperative day 3, and the patient was discharged home.
- Ethics statement
- This study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent for publication of the research details and clinical images was obtained from the patient’s legal guardian and the manuscript was reviewed by the privacy coordinator prior to submission.
CASE REPORT
- The Eastern Association for the Surgery of Trauma (EAST) guidelines recommend that the management of penetrating injuries isolated to the right upper abdominal quadrant includes observation or surgical intervention depending on the patient’s vital signs and physical examination findings. Patients with stable vital signs, a reliable examination, and minimal to no abdominal tenderness can be observed [3]. Although our patient had an isolated right upper quadrant abdominal penetrating injury, he presented with abdominal tenderness, evidence of pericholecystic fluid, and concerns for intestinal injury; thus, surgical exploration was warranted.
- Advances in minimally invasive surgery have allowed patients that are hemodynamically normal to undergo diagnostic laparoscopy instead of open abdominal exploration. This technique has been shown to be safe and practical in selected patients when performed by experienced surgeons [4,5]. It enables a complete evaluation of intra-abdominal viscera, reduces the incidence of nontherapeutic operations, and allows a therapeutic intervention when needed [5]. Laparoscopy allowed us to carefully evaluate the colonic hepatic flexure and surrounding structures, ruling out colonic injury without the need for open exploration and allowing identification of the gallbladder wall injury and bile spillage. Additionally, minimizing the size of the surgical scars had a positive psychological impact on the patient’s experience.
- Simple gallbladder contusions or partial avulsions can be treated conservatively in patients who are hemodynamically stable and have minimal symptoms [1]. However, in the setting of a penetrating injury, the most likely injury is a gallbladder wall perforation or laceration, for which laparoscopic cholecystectomy is recommended [1,6]. Suturing of the gallbladder perforation was advocated in the past, but it carries risks of cholecystitis, re-rupture, wall necrosis, and promoting calculus formation [7].
- A recent review of traumatic gallbladder perforation in children reported eight cases of blunt trauma causing gallbladder perforation that were managed with cholecystectomy with favorable outcomes [1]. Five of the eight operations were done in a laparoscopic fashion. Laparoscopic cholecystectomy can be considered a feasible treatment option for stable pediatric patients with penetrating gallbladder injuries.
DISCUSSION
-
Author contributions
Conceptualization: all authors; Data curation: all authors; Formal analysis: all authors; Methodology: all authors; Project administration: RJH; Writing–original draft: NCC; Writing–review & editing: SS, DRM, CD, RJH. All authors read and approved the final manuscript.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
The authors did not receive any financial support for this study.
-
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.
ARTICLE INFORMATION

- 1. Le MT, Herrmann J, Groth M, Reinshagen K, Boettcher M. Traumatic gallbladder perforation in children: case report and review. Rofo 2021;193:889–97. ArticlePubMed
- 2. Marriott FP. A case of a penetrating injury of the gall bladder due to a knife wound in a nine year old boy. Ulster Med J 1966;35:100–4. PubMedPMC
- 3. Como JJ, Bokhari F, Chiu WC, et al. Practice management guidelines for selective nonoperative management of penetrating abdominal trauma. J Trauma 2010;68:721–33. ArticlePubMed
- 4. Mahmoud MA, Daboos MA, Bayoumi AS, et al. Role of minimally invasive surgery in management of penetrating abdominal trauma in children. Eur J Pediatr Surg 2021;31:353–61. ArticlePubMed
- 5. Pau L, Navez J, Cawich SO, Dapri G. Laparoscopic management of blunt and penetrating abdominal trauma: a single-center experience and review of the literature. J Laparoendosc Adv Surg Tech A 2021;31:1262–8. ArticlePubMed
- 6. Egawa N, Ueda J, Hiraki M, et al. Traumatic gallbladder rupture treated by laparoscopic cholecystectomy. Case Rep Gastroenterol 2016;10:212–7. ArticlePubMedPMCPDF
- 7. Jaggard MK, Johal NS, Choudhry M. Blunt abdominal trauma resulting in gallbladder injury: a review with emphasis on pediatrics. J Trauma 2011;70:1005–10. ArticlePubMed
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-


- Related articles
-
- Massive traumatic abdominal wall hernia in pediatric multitrauma in Australia: a case report
- Penetrating chest trauma from a “less lethal” bean bag in the United States: a case report
- Isolated penetrating gluteal stab injury with uncontrolled bleeding in Türkiye: a case report
- Blunt abdominal trauma resulting in pancreatic injury in a pediatric patient in Australia: a case report
- Repair of traumatic flank hernia with mesh strip suture: a case report

