
Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(4); 2023 > Article
-
Original Article
A decade of treating traumatic sternal fractures in a single-center experience in Korea: a retrospective cohort study -
Na Hyeon Lee, MD
 , Seon Hee Kim, MD, Jae Hun Kim, MD, Ho Hyun Kim, MD, Sang Bong Lee, MD, Chan Ik Park, MD, Gil Hwan Kim, MD, Dong Yeon Ryu, MD, Sun Hyun Kim, MD
, Seon Hee Kim, MD, Jae Hun Kim, MD, Ho Hyun Kim, MD, Sang Bong Lee, MD, Chan Ik Park, MD, Gil Hwan Kim, MD, Dong Yeon Ryu, MD, Sun Hyun Kim, MD -
Journal of Trauma and Injury 2023;36(4):362-368.
DOI: https://doi.org/10.20408/jti.2023.0027
Published online: November 30, 2023
- 671 Views
- 32 Download
Department of Trauma and Surgical Critical Care, Biomedical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, Busan, Korea
- Correspondence to: Seon Hee Kim, MD Department of Trauma and Surgical Critical Care, Biomedical Research Institute, Pusan National University Hospital, Pusan National University School of Medicine, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea Tel: +82-51-240-7369 Email: ksh810427@naver.com
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- Clinical reports on treatment outcomes of sternal fractures are lacking. This study details the clinical features, treatment approaches, and outcomes related to traumatic sternal fractures over a 10-year period at a single institution.
-
Methods
- A retrospective cohort study was conducted of patients admitted to a regional trauma center between January 2012 and December 2021. Among 7,918 patients with chest injuries, 266 were diagnosed with traumatic sternal fractures. Patient data were collected, including demographics, injury mechanisms, severity, associated injuries, sternal fracture characteristics, hospital stay duration, mortality, respiratory complications, and surgical details. Surgical indications encompassed emergency cases involving intrathoracic injuries, unstable fractures, severe dislocations, flail chest, malunion, and persistent high-grade pain.
-
Results
- Of 266 patients with traumatic sternal fractures, 260 were included; 98 underwent surgical treatment for sternal fractures, while 162 were managed conservatively. Surgical indications ranged from intrathoracic organ or blood vessel injuries necessitating thoracotomy to unstable fractures with severe dislocations. Factors influencing surgical treatment included flail motion and rib fracture. The median length of intensive care unit stay was 5.4 days (interquartile range [IQR], 1.5–18.0 days) for the nonsurgery group and 8.6 days (IQR, 3.3–23.6 days) for the surgery group. The median length of hospital stay was 20.9 days (IQR, 9.3–48.3 days) for the nonsurgery group and 27.5 days (IQR, 17.0 to 58.0 days) for the surgery group. The between-group differences were not statistically significant. Surgical interventions were successful, with stable bone union and minimal complications. Flail motion in the presence of rib fracture was a crucial consideration for surgical intervention.
-
Conclusions
- Surgical treatment recommendations for sternal fractures vary based on flail chest presence, displacement degree, and rib fracture. Surgery is recommended for patients with offset-type sternal fractures with rib and segmental sternal fractures. Surgical intervention led to stable bone union and minimal complications.
- Background
- Sternal fractures resulting from trauma are relatively rare, representing 3% to 8% of all blunt trauma cases [1–4]. The most common mechanism of injury is direct blunt force to the anterior chest, typically from traffic accidents, with falls being the next most common cause [1,4–6]. The body of the sternum is the most common site of these fractures, while fractures of the manubrium or xiphoid process are comparatively rare [2,4,7]. The mortality or morbidity associated with sternal fractures is determined not by the fracture itself, but by the severity of the accompanying injury, with mortality rates varying between 4% and 45% [2,4,8].
- Most cases are managed with conservative treatment. However, conditions such as chronic nonunion, severe pain that impacts breathing, displacement, overlapping fractures that cannot be rectified by closed reduction, and sternal instability are indications for surgical treatment [3]. The most common surgical treatment is open reduction and internal fixation (ORIF) using a plate. This method is recognized as the most effective for stabilizing the anterior chest wall, preventing impaired bone healing, and avoiding other complications [4,5,9].
- Objectives
- Limited data have been published on the long-term experience of a single center regarding the treatment and outcomes of sternal fractures. Consequently, the objective of this study was to present the clinical aspects, treatment, and outcomes of traumatic sternal fractures over 10 years at a single center.
INTRODUCTION
- Ethics statement
- This study was approved by the Institutional Review Board of Pusan National University Hospital (No. H-2304-021-126). The requirement for informed consent was waived due to the retrospective nature of the study. This study was conducted in compliance with the principles of the Declaration of Helsinki.
- Study design and participants
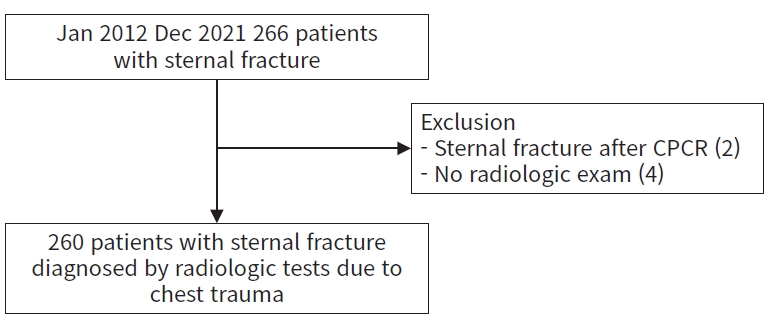
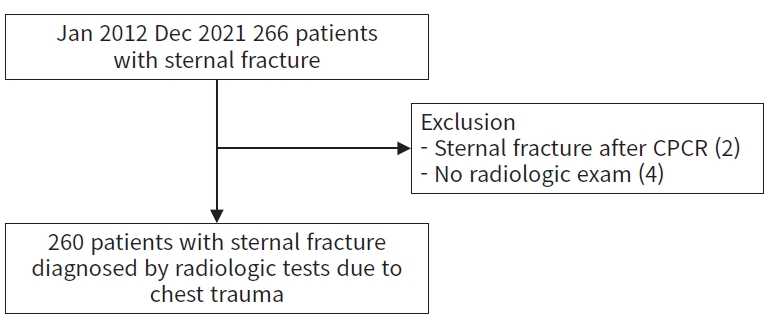
- This retrospective cohort study involved patients admitted to a regional trauma center between January 2012 and December 2021. Using the hospital’s inpatient inquiry system, we identified 7,918 patients with chest injuries who had been admitted to the Regional Trauma Center of Pusan National University Hospital (Busan, Korea). Among these patients, we reviewed the medical records of 266 who were diagnosed with traumatic sternal fractures. The criteria for inclusion in the study were as follows: (1) a sternal fracture had to be registered as a diagnosis and be searchable in the medical records; and (2) the location of the sternal fracture had to be confirmable through computed tomography (CT) or radiography. We excluded patients who had sustained a sternal fracture due to cardiopulmonary cerebral resuscitation and those for whom sternal fractures could not be confirmed because the imaging data were not recorded (Fig. 1).
- The data collected included patient demographics, injury mechanism, injury severity, intrathoracic and extrathoracic injuries, sternal fracture characteristics, duration of hospital and intensive care unit (ICU) stays, in-hospital mortality rates, respiratory complications, and surgical features of the sternal fracture.
- Diagnosis of sternal fractures and surgical indications
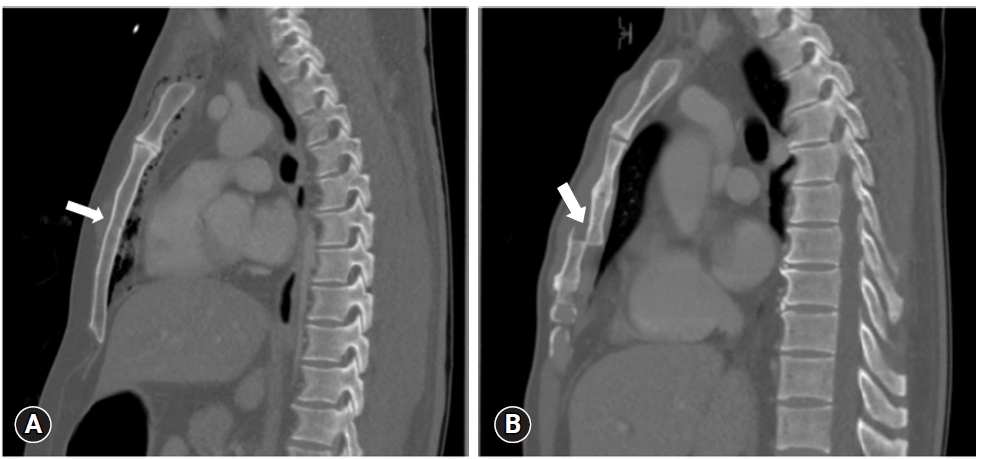
- The diagnosis was established using chest CT, either non–contrast-enhanced or contrast-enhanced, or sternal lateral radiography. Based on the degree of displacement, the condition was categorized as either nondisplaced, offset, or displaced (Fig. 2).
- Surgical indications included the following: (1) instances in which emergency surgery was conducted via thoracotomy due to injuries to intrathoracic organs or blood vessels, and where the patient’s condition allowed for the concurrent correction of the sternal fracture; (2) unstable fractures that were accompanied by severe dislocations or exhibited an offset of 50% or more; (3) instances of flail chest associated with respiratory failure; (4) observed malunion (nonunion or abnormal union) of the fractures; and (5) reports of pain with a numeral rating scale of 6 or higher that persisted for more than 72 hours despite adequate pain control.
- The surgical procedure was conducted based on ORIF, utilizing plates inserted via a median vertical incision between the sternal notch and the tip of the xiphoid process. In certain instances, wire fixation was also implemented. Following surgery, lateral radiography of the sternum was conducted. If sternal lateral radiography was not available, chest CT was performed instead.
- Intrathoracic and extrathoracic injuries
- The associated intrathoracic injuries included the following: (1) damage to the heart, aorta, or other arteries; (2) lung contusion; (3) hemothorax and/or pneumothorax; (4) rib fracture; and (5) retrosternal hematoma. Injuries classified as extrathoracic were those identified with an Abbreviated Injury Scale (AIS) score of 3 or higher, encompassing injuries to the head and neck, face, abdomen, and extremities.
- Statistical analysis
- When appropriate, summary statistics were presented as medians with interquartile ranges (IQRs) or as means with standard deviations. Categorical variables were expressed as numbers and percentages. To compare the frequencies of categorical variables between groups, the chi-square and Fisher exact tests were employed. The Mann-Whitney U-test and Wilcoxon rank-sum test were utilized to compare the mean values of continuous variables. A P-value of less than 0.05 was considered to indicate statistical significance. Data analysis was conducted using IBM SPSS ver. 22.0 (IBM Corp).
METHODS
- Of the 266 patients diagnosed with sternal fractures, we excluded two patients who had sustained these fractures following cardiopulmonary resuscitation due to illness, as well as four patients for whom imaging data were not available. The most common mechanism of injury was motor vehicle accidents, followed by falls and crushing injuries. The Injury Severity Score was categorized as mild (<9), moderate (9–15), severe (16–25), or profound (>25). The largest number of patients fell into the severe injury category, but the difference was not statistically significant (Table 1).
- Of the 260 patients included in this study, 98 underwent surgical procedures for sternal fractures, while the remaining 162 received conservative treatment. Flail motion was observed in 96 patients, with 93 of these patients also presenting with rib fractures. Among the three patients without rib fractures, two exhibited flail motion with a fracture gap that had increased compared to the initial phase, and one patient had a segmental fracture of the sternal body. Regarding intrathoracic injuries, damage to the heart, aorta, or other arteries was confirmed in 20 patients from the surgery group and 14 from the nonsurgery group.
- The median duration of ICU stay across all patients was 6.6 days (IQR, 2.0–21.3 days). For the surgery group, the median stay was 8.6 days (IQR, 3.3–23.6 days), while for the nonsurgery group, it was 5.4 days (IQR, 1.6–18.0 days). However, this difference was not statistically significant. Furthermore, the median length of hospital stay was 27.5 days (IQR, 17.0–58.0 days) for the surgery group and 20.0 days (IQR, 9.3–43.8 days) for the nonsurgery group. This difference was statistically significant. No significant difference was observed between the groups with regard to in-hospital mortality and respiratory complications, such as pneumonia. In a multivariate analysis examining the incidence of pneumonia following surgery for sternal fracture without rib fracture, none of the patients who underwent surgery developed pneumonia (Table 2). However, pneumonia did occur in seven of the 60 patients (11.7%) who did not undergo surgery (P=0.192). In addition, no significant difference was found in the occurrence of pneumonia between the surgery and nonsurgery groups with an AIS score of less than 3 for head and neck injuries; this condition arose in nine (40.9%) and 20 patients (36.4%), respectively (P=0.911).
- Fractures were the most frequently observed injury, although sternomanubrial joint dislocation was noted in three instances, and a combination of dislocation and fracture was seen in three other cases. The sternal body was the most common site of sternal fracture, followed by the manubrium. Regarding the extent of displacement in sternal fractures, the offset type was the most frequently observed, occurring in 111 patients. Among these 111 patients with offset-type fractures, 19 exhibited an offset of 50% or more. In the group of patients who underwent surgery, the offset type was most frequently seen, followed by the displaced type. In contrast, among the patients who did not undergo surgery, the nondisplaced type was most common, observed in 91 patients, while the offset type was seen in 62 patients (Table 3).
- A total of 90 patients underwent ORIF, with three patients receiving wire fixation and three patients receiving a combination of wire and plate fixation. One patient treated with ORIF continued to experience chest wall instability, leading to the insertion and subsequent removal of a Nuss bar. One patient underwent resection of the xiphoid process. None of the patients who underwent surgery exhibited sternal instability or incomplete bone union during outpatient follow-up. Twenty patients reported experiencing prolonged pain, and two patients received treatment for wound complications. Fixation removal was carried out in 18 patients, with chest tightness being the most common reason for removal, reported by nine patients. This was followed by screw loosening in five patients and infection in one patient. The average duration from the initial operation to removal was 460 days. No patients encountered issues with bone union. The average duration from admission to surgery was 6 days, and the average duration from hospitalization to discharge postsurgery was 43 days (Table 4).
RESULTS
- Sternal fractures can typically be managed through conservative treatment without surgery. However, surgical intervention is indicated when unstable fractures are coupled with severe dislocations, or in cases of flail chest accompanied by respiratory failure. In such instances, if surgical treatment is not undertaken, an increased risk exists of respiratory distress and a prolonged period of ventilator application. This heightens the likelihood of respiratory complications, such as pneumonia, particularly as the duration of the ICU stay is extended. Therefore, it is crucial to appropriately identify patients who would benefit from either surgical or conservative treatments and administer the corresponding treatment accordingly [4].
- Sternal fixation surgery has seen a recent exponential increase in performance, yet the indications for its application remain unestablished [10]. Our study revealed no significant difference in the mean Injury Severity Score between surgical and nonsurgical groups. However, the surgery group displayed a higher incidence of intrathoracic injuries, including heart, aorta, or other arterial injuries, and flail chest. This suggests that surgical sternal fixation may be indicated when heart or thoracic vessel injuries and multiple rib fractures necessitate surgery. Displacement can be classified into nondisplaced, offset, and displaced categories [11]. At our center, indications for surgery included either an offset of more than 50% or displacement. Of the 111 patients with offset displacement, 19 had an offset of 50% or more. Among these, six patients with flail motion underwent ORIF, all of whom had rib fractures. The remaining 13 patients did not exhibit flail motion, and only four of them had rib fractures. Of the six patients who underwent surgery without flail motion, one experienced a xiphoid resection due to abnormal union, and five had surgery due to persistent pain and chest discomfort. Of the 92 patients with an offset of less than 50%, 33 had a flail chest, of whom 32 had rib fractures and one had a segmental fracture of the sternal body. Therefore, in cases of offset displacement, the presence of a rib fracture contributed more to the occurrence of flail motion than the degree of displacement. This is further supported by the fact that of 96 patients exhibiting flail motion, 93 had rib fractures. In cases of flail motion without rib fractures, the displacement was not severe, but a segmental fracture of the sternum was observed. Thus, when deciding on surgical treatment, it is more appropriate to consider not only the degree of displacement but also the presence of flail motion as an indication for surgery.
- In cases of anterior flail chest due to a sternal fracture accompanied by bilateral multiple rib fractures, particularly when fixation of the costal cartilage or sternocostal junction is necessary, conventional ORIF may not be easily executed. Under such circumstances, fixation using a Nuss bar can be employed [12]. In the present study, within the ORIF group, the flail motion persisted in one instance even after ORIF was performed. For this patient, fixation was carried out on the right fourth sternocostal junction and costal cartilage using sternum ORIF. A Nuss bar was inserted 1 week following the ORIF procedure and was removed 1 year after its insertion.
- During conservative treatment, it is crucial to manage pain and maintain pulmonary hygiene to prevent respiratory complications, such as atelectasis and pneumonia [4]. Pain management can be achieved through various methods, such as patient-controlled epidural analgesia. This is particularly beneficial for patients who struggle to manage pain with oral, intravenous, or intramuscular analgesia; those with bilateral or numerous fractures; or those at an elevated risk of respiratory complications due to advanced age [13]. In our facility, we typically use a combination of acetaminophen and tramadol as the primary oral analgesia. Depending on the severity of the pain, we may add oral pregabalin to the regimen, and we resort to patient-controlled epidural analgesia when pain becomes unmanageable with oral analgesia. Additionally, we routinely implement respiratory rehabilitation in collaboration with the Department of Rehabilitation Medicine. Even in the absence of significant intrathoracic organ or blood vessel injury on a chest CT scan, the potential remains for cardiac contusion. Therefore, laboratory tests such as evaluation of cardiac markers, electrocardiography, and echocardiography may be necessary to assess cardiac function [14]. For such patients at our facility, we monitor cardiac markers and electrocardiography serially over a 72-hour period, and we also perform echocardiography.
- Limitations
- This study had certain limitations. First, it was a small-scale study conducted at a single center. Second, the study did not solely focus on patients with sternal fractures, but rather included all trauma patients who had sustained such fractures. As a result, it was challenging to pinpoint complications specifically attributable to sternal fractures, given that the length of ICU stay, the total duration of hospital stay, and the incidence rate of respiratory complications could be influenced by concurrent injuries unrelated to the sternal fracture. Finally, in the context of trauma, patients are commonly lost to outpatient follow-up due to transfer to another hospital or nonattendance after recovery. Consequently, it is difficult to ascertain long-term outcomes in these patients.
- Conclusions
- Surgery may be recommended for patients exhibiting flail chest in conjunction with the offset type of sternal fracture and accompanying rib fractures, or in patients with segmental sternal fracture. Furthermore, given that trauma patients often sustain multiple injuries, identifying significant differences in mortality and morbidity specifically attributable to sternal fracture surgery can be challenging. Therefore, a study involving a more standardized and homogeneous group is required.
DISCUSSION
-
Author contributions
Conceptualization: Seon Hee K, GHK, JHK; Data curation: JHK, SBL, CIP; Formal analysis: CIP, DYR, NHL; Funding: Seon Hee K; Methodology: HHK, DYR, Sun Hyun K; Project administration: Seon Hee K, NHL, SBL; Visualization: SBL, GHK, JHK, DYR; Writing–original draft: NHL, Seon Hee K, Sun Hyun K; Writing–review & editing: NHL, HHK, CIP. All authors read and approved the final manuscript.
-
Conflicts of interest
Seon Hee Kim and Ho Hyun Kim are Editorial Board members of the Journal of Trauma and Injury, but were not involved in the peer reviewer selection, evaluation, or decision process of this article. The authors have no other conflicts of interest to declare.
-
Funding
This study was supported by a 2-year research grant from Pusan National University.
-
Data availability
Data analyzed in this study are available from the corresponding author upon reasonable request.
ARTICLE INFORMATION
| Variable | Surgery group (n=18) | Nonsurgery group (n=60) | P-value |
|---|---|---|---|
| Without rib fracturea) | 0 | 7 (11.7) | 0.192 |
| Head and neck (AIS <3)b) | 9 (40.9) | 20 (36.4) | 0.911 |
- 1. Zhao Y, Yang Y, Gao Z, Wu W, He W, Zhao T. Treatment of traumatic sternal fractures with titanium plate internal fixation: a retrospective study. J Cardiothorac Surg 2017;12:22. ArticlePubMedPMCPDF
- 2. Athanassiadi K, Gerazounis M, Moustardas M, Metaxas E. Sternal fractures: retrospective analysis of 100 cases. World J Surg 2002;26:1243–6. ArticlePubMedPDF
- 3. Harston A, Roberts C. Fixation of sternal fractures: a systematic review. J Trauma 2011;71:1875–9. ArticlePubMed
- 4. Klei DS, de Jong MB, Oner FC, Leenen LP, van Wessem KJ. Current treatment and outcomes of traumatic sternal fractures-a systematic review. Int Orthop 2019;43:1455–64. ArticlePubMedPDF
- 5. Byun CS, Park IH, Hwang WJ, Lee Y, Cho HM. Analysis of sternal fixation results according to plate type in sternal fracture. Korean J Thorac Cardiovasc Surg 2016;49:361–5. ArticlePubMedPMC
- 6. Ahmad K, Katballe N, Pilegaard H. Fixation of sternal fracture using absorbable plating system, three years follow-up. J Thorac Dis 2015;7:E131–4. PubMedPMC
- 7. Schulz-Drost S, Oppel P, Grupp S, et al. The oblique fracture of the manubrium sterni caused by a seatbelt: a rare injury? Treatment options based on the experiences gained in a level I trauma centre. Int Orthop 2016;40:791–8. ArticlePubMedPDF
- 8. Knobloch K, Wagner S, Haasper C, et al. Sternal fractures occur most often in old cars to seat-belted drivers without any airbag often with concomitant spinal injuries: clinical findings and technical collision variables among 42,055 crash victims. Ann Thorac Surg 2006;82:444–50. ArticlePubMed
- 9. Schulz-Drost S, Oppel P, Grupp S, et al. Surgical fixation of sternal fractures: preoperative planning and a safe surgical technique using locked titanium plates and depth limited drilling. J Vis Exp 2015;(95):e52124ArticlePubMed
- 10. Doyle JE, Diaz-Gutierrez I. Traumatic sternal fractures: a narrative review. Mediastinum 2021;5:34. ArticlePubMedPMC
- 11. Edwards JG, Clarke P, Pieracci FM, et al. Taxonomy of multiple rib fractures: results of the chest wall injury society international consensus survey. J Trauma Acute Care Surg 2020;88:e40–5. ArticlePubMed
- 12. Kim D, Yoon SK, Lee GD, Kim DK. Nuss procedure for surgical stabilization of anterior flail chest with mechanical ventilation weaning failure: a case report. J Chest Surg 2022;55:183–7. ArticlePubMedPMC
- 13. Kim M, Moore JE. Chest trauma: current recommendations for rib fractures, pneumothorax, and other injuries. Curr Anesthesiol Rep 2020;10:61–8. ArticlePubMedPMCPDF
- 14. Khoriati AA, Rajakulasingam R, Shah R. Sternal fractures and their management. J Emerg Trauma Shock 2013;6:113–6. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-

- Related articles
-
- One year of treating patients with open fractures of the lower extremity in a new military trauma center in Korea: a case series
- Pediatric blunt pancreatic trauma at a single center in Korea: a retrospective review from 2007 to 2022
- Relationship between sonorheometry parameters and laboratory values in a critical care setting in Italy: a retrospective cohort study
- Management of a traumatic avulsion fracture of the occipital condyle in polytrauma patient in Korea: a case report
- Effect of use and type of helmet on occurrence of traumatic brain injuries in motorcycle riders in Korea: a retrospective cohort study

