
Articles
- Page Path
- HOME > J Trauma Inj > Volume 30(4); 2017 > Article
-
Original Article
Prognosis of Pulmonary Function in Patients with Multiple Rib Fractures - Hee Beom Park, M.D.1, Sung Youl Hyun, M.D.2, Jin Joo Kim, M.D.1, Yeon Sik Jang, M.D.1
-
Journal of Trauma and Injury 2017;30(4):179-185.
DOI: https://doi.org/10.20408/jti.2017.30.4.179
Published online: December 30, 2017
- 10,707 Views
- 100 Download
- 3 Crossref
1Department of Emergency Medicine, Gachon University Gil Medical Center, Incheon, Korea
2Department of Trauma Surgery, Gachon University Gil Medical Center, Incheon, Korea
- Correspondence to: Sung Youl Hyun, M.D., Department of Trauma Surgery, Gachon University Gil Medical Center, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea, Tel: +82-32-460-3015, Fax: +82-32-460-3019, E-mail: sungyoul@gilhospital.com
• Received: August 22, 2017 • Revised: October 7, 2017 • Accepted: October 20, 2017
Copyright © 2017 The Korean Society of Trauma
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- Rib fracture is the most common complication of blunt thoracic trauma. We investigated the effect of rib fracture on pulmonary function in the conservatively treated patients.
-
Methods
- From January 2000 to February 2017, we reviewed the records of 72 patients with rib fracture and pulmonary function tests were performed. According to the number of rib fractures, patients were classified into two groups: less than six fractured ribs (group A) and more than six fractured ribs (group B). The groups were compared concerning demographics, underlying diseases, associated thoracic injuries, surgery, mechanical ventilator times, days spent in the intensive care unit and pulmonary function test.
-
Results
- There were no statistically significant differences in the demographic data between the two groups. Mean hospitalization was 13.5 days in group A and 27.0 days in group B (p<0.001). There was no statistically significant difference between the two groups in the pulmonary function test.
-
Conclusions
- We conclude that pulmonary function is restored by conservative treatment in patients with rib fractures even if the number of rib fractures increases. In patients with multiple rib fractures, studies comparing open rib fixation and conservative treatment of long term pulmonary function are required.
- Thoracic traumas comprise 10–15% of all traumas and are the cause of death in 25% of all trauma-related fatalities [1]. The most common type of thoracic trauma is decelerating injuries caused by collisions like traffic accidents. Trauma related to accidents like falls and slip down has also increased [2]. Rib fractures are the most common bony injuries in thoracic trauma and are diagnosed in approximately 50% of patients admitted to the hospital following thoracic trauma. Rib fractures can be markers of potential internal injury. The principal diagnostic goal with clinically suspected rib fractures is the detection of significant associated complications, such as hemopneumothorax, pulmonary contusion, intra-abdominal injury, or major vascular injury. The pain of rib fractures can greatly interfere with ventilation, cause splinting and atelectasis, and prolong the time for weaning from ventilator support. Patients with multiple fractured ribs will often have difficulty coughing or adequately clearing secretions, and should be considered for 24 to 48 hours of observation unit admission [3]. The presence of three or more rib fractures has been associated with increased mortality and duration of care in intensive care units (ICUs) and hospitals [4]. Increasing number of rib fractures correlates directly with increasing pulmonary morbidity (atelectasis, pneumonia) and mortality [5–7].
- This morbidity and mortality associated with rib fractures is caused by three main problems: hypoventilation due to pain, impaired gas exchange in damaged lung underlying the fractures, and altered breathing mechanics. An injury severe enough to fracture ribs will invariably cause a substantial contusion to the underlying lung. The damaged lung is poorly compliant and will not take part in gas exchange [8]. Pulmonary contusion usually resolves without causing permanent complications [9]. However, it may also have long-term adverse effects on pulmonary function. Fibrosis of the lungs can occur, resulting in dyspnea (shortness of breath), low blood oxygenation, and reduced functional residual capacity after the injury [10]. Contusion can also permanently reduce the compliance of the lungs [11].
- There are not many studies on the effect of rib fracture on pulmonary function. We investigated the effect of rib fracture on pulmonary function in the conservatively treated patients.
INTRODUCTION
- Study design and population
- From January 2000 to February 2017, we retrospectively reviewed the records of patients with rib fracture treated in our university hospital emergency medical center. The center has approximately 90,000 patient visits annually. Of the reviewed patients, 120 had undergone pulmonary function tests 6–23 months following discharge. The included were over 18 years of age and had experience blunt trauma-related rib fracture. Exclusion criteria were lack of necessary medical records, absence of pulmonary function testing, abbreviated injury scale score≥3 for each body region, except the thorax, and history of mechanical ventilation or ICU stay due to damage to the abdomen and other organs. Finally, 72 patients were enrolled (Fig. 1).
- Indications for admission were patients who those with more than three rib fractures, clinical symptoms including dyspnea and chest pain, and significant associated complications like hemopneumothorax and pulmonary contusion.
- Data collection
- Electronic medical records and radiographs of each patient were retrospectively reviewed by one emergency medicine doctor. Patients were classified into two groups based on the extent of rib fracture: less than six ribs (group A) and more than six ribs (group B). Variables included number of rib fractures, age, sex, underlying diseases, associated thoracic injuries, surgery, mechanical ventilator days, ICU days, and pulmonary function test.
- Outcomes
- The primary outcome was hospitalization in days including ICU days. Secondary outcome included the pulmonary function of patients with rib fractures. Pulmonary function tests were performed following the American Thoracic Society/European Respiratory Society guidelines by technicians experienced in pulmonary function testing. Spirometry was performed according to current recommendations [12,13]. Restrictive pattern was defined as a measured forced vital capacity (FVC) <80% of the predicted value for the patient. Obstructive pattern was defined as a measured forced expiratory volume in 1 second (FEV1)/FVC and FEV1<80% of the predicted value for the patient.
- Statistical analyses
- Univariate analyses involved the chi-squared test for the analysis of categorical variables and the Wilcoxon rank-sum test for the analysis of continuous variables. Multivariate analyses used logistic regression and multiple regression. Dependent variables in logistic regression were mechanical ventilator care, FEV1, FVC, and ICU admission days. All statistical analyses were performed using STATA version 13 (Stata Corp., College Station, TX, USA). The significance level was 0.05 (p-value). Quantitative data are presented as the mean±standard deviation.
METHODS
- Of the 72 patients 11 (15%) were women and 61 (85%) were men. The mean age was 51.2±12.0 (range 19 to 83 years). There were 22 (30%) patients in group A and 50 (70%) in group B. There were no statistically significant differences in sex ratio, age, and underlying lung disease between the two groups.
- Group B patients were more likely to have been treated using closed thoracostomy than group A (50% vs. 90%, p=0.001). There was no statistically significant difference between the group A and B concerning rib fixation (n=0, 0% vs. n=5, 10.0%). The mean hospitalization was 13.5 days in group A and 27.0 days in group B (p<0.001). ICU admission was one (4.5%) in group A and 37 (74.0%) in group B. The incidence of ICU admission and ventilator application was significantly higher in group B (both p<0.001). During the hospital stay, pneumonia and acute respiratory distress syndrome (ARDS) were observed in two groups. In group A, there were 0 cases of pneumonia, ARDS among 22 patients (0%). Group B also had complications in 0 out of 50 patients (0%). FVC was <80% in 6 patients (27.3%) in group A and 24 patients (48%) in group B. FEV1 was <80% in 8 patients (36.4%) in group A and 21 patients (42%) in group B. The FEV1/FVC was <80% in six (27.3%) group A patients and six (12.0%) group B patients. There was no statistically significant difference between the two groups in the pulmonary function test. In the total population, FEV1/FVC was ≥80% in 60 (83.3%) patients and FEV1 was ≥80% in 43 (59.7%) patients (Table 1).
- The mean duration of mechanical ventilation was 0 days in group A and 4 days in group B. The mean ICU stay was 0.1 days in group A and 6.3 days in group B (p<0.001).
- Univariate analysis revealed that factors affecting ICU admission were ≥6 rib fractures (β=5.369, p<0.001) and flail chest (β=8.583, p<0.001). In multivariate analysis, factors affecting ICU admission were also ≥6 rib fractures (adjusted β=4.053, p=0.001) and flail chest (adjusted β=7.924, p<0.001) (Table 2).
- No factor affected pulmonary function (Table 3).
RESULTS
- A recent study highlighted the detrimental effects of increasing number of rib fractures and age. The authors demonstrated that patients older than 65 years with more than four fractures had higher morbidity and mortality [14]. Another study reported that patients older than 45 years of age with more than four rib fractures are at risk of prolonged ICU stays, ventilator days, and overall hospital days [15]. Increasing number of rib fractures has been correlated directly with increasing pulmonary morbidity and mortality [5]. In this study, we also demonstrated that patients with more than six rib fractures exhibit prolonged ICU stays, ventilator days, and overall hospital days. Mechanical ventilator apply was performed in 31 patients. The reason for the intubation was as follows. 11 were due to flail chest and 19 were due to lung contusion. The other was performed because of diaphragm injury. Table 1 shows that flail chest and lung contusion more occurred in group B. Compared with group A, lung contusion and flail chest occurred frequently in group B, Mechanical ventilation application was performed more than group A. The mean duration of mechanical ventilation was 4 days in group B. Lung contusion was the most common reason for longer duration of mechanical ventilation when patients were applied for more than 4 days (13 patients, 5.8 days). The next was flail chest (5 patients, 5.8 days).
- Flagel et al. [5] found that when six or more ribs are fractured, pulmonary morbidity and flail chest are increased. It would have a significant effect on the pulmonary function outcome. So we divided them into two groups based on six. In this study, increasing number of rib fractures was not associated with pulmonary function previous study that reported improvement in pulmonary function tests after 6 to 18 months [16]. Other authors reported that in a cohort of 13 survivors of severe thoracic trauma with lung contusion, substantial physiological recovery was evident with good pulmonary function tests [17]. Surgical fixation of ribs can be carried out as a first-line therapeutic option for bilateral rib fractures or flail segments without significant complications if the risk factors associated with mortality are carefully considered [18]. The authors also opined that, with a view of restoring pulmonary function as well as chest wall configuration, early operative stabilization of the ribs can be more helpful than conventional treatment for patients with multiple rib fractures. Early restoration of the chest wall integrity and respiratory functions prevents restrictive impairment of pulmonary functions, as proven by the total lung capacity values surgically treated patients presented 6 months postoperatively, which were all significantly higher than 85% of the predicted value [19]. The indications for fixation of ribs remain controversial mostly because of a lack of adequate studies comparing operative and non-operative treatment. In this study, the majority of patients with multiple rib fractures were treated without rib fixation. Only five patients underwent rib fixation, and fixation was performed by suture fixation. In a previous study, rib fixation was performed using a metal plate. In plate fixation, firm fixation might not be achieved, creating a risk of dislocation. Complications, such as osteomyelitis, are related to fixation to the bone marrow through the ribs. The patients enrolled in this study tended to recover pulmonary function without rib fixation. The collective findings highlight the need for more studies on the surgical reduction of rib fracture.
- The primary limitation for this study is related to selection bias, because this study was conducted in a single center and had limited sample size. The small number of patients makes it difficult to prove that variables affect morbidity and pulmonary function. Another significant limitation is inherent to the retrospective nature of this study. Because this study has a retrospective design, patients underwent pulmonary function tests at different times. Prospective studies including serial pulmonary function tests are needed to definitively determine the effect of rib fractures on long-term outcome. The purpose of this study was to investigate the effect of the number of rib fractures on pulmonary function simply. Diffusing capacity of the lungs for carbon monoxide (DLCO) was needed to examine the effect of lung fibrosis caused by sequelae of lung contusion on pulmonary function. But, DLCO could not be performed in all patients. And pleural adhesion, thickening, and deformity were excluded because of the lack of accurate radiologic findings due to retrospective study limitations.
DISCUSSION
- In patients with lung contusion or flail chest, early conservative treatment could restore patients without any specific complications. We conclude that pulmonary function is restored by conservative treatment in patients with rib fractures even if the number of rib fractures increases. In patients with multiple rib fractures, more research is needed on factors that can be associated with pulmonary function, such as pain, pleural sequelae and diffusion capacity. Also studies comparing open rib fixation and conservative treatment of long term pulmonary function are required.
CONCLUSION
Fig. 1Flow chart of study subjection selection. PFT: pulmonary function test, AIS: abbreviated injury scale.
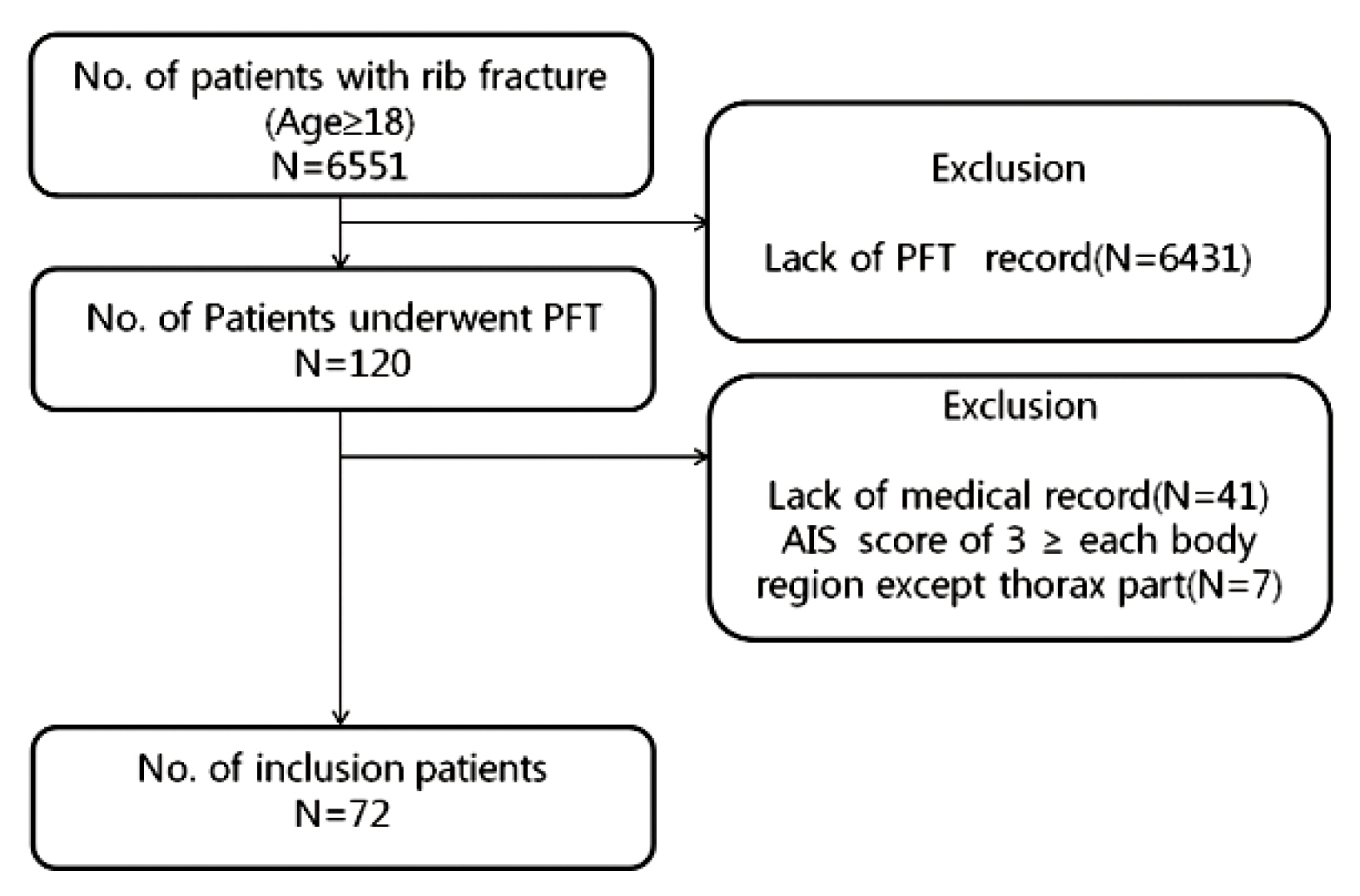
Table 1Characteristics of patients with rib fractures
Table 2Factors related to ICU days
| Univariate | Stepwise backward regression | |||
|---|---|---|---|---|
|
|
|
|||
| Beta | p-value | Adjusted beta | p-value | |
| More than 6 ribs | 5.369 | <0.001 | 4.053 | 0.001 |
|
|
||||
| Sex | −0.135 | 0.938 | ||
|
|
||||
| Age | 0.055 | 0.339 | 0.082 | 0.077 |
|
|
||||
| Associated thoracic injurya | 2.183 | 0.014 | ||
|
|
||||
| Flail chest | 8.583 | <0.001 | 7.924 | <0.001 |
|
|
||||
| Lung contusion | 2.989 | 0.031 | ||
|
|
||||
| Underlying lung disease | −2.410 | 0.335 | ||
|
|
||||
| Bilateral rib fractures | 3.157 | 0.027 | ||
Table 3Factors related to FEV1 and FEV1/FVC
| FEV1 | FEV1/FVC | |||
|---|---|---|---|---|
|
|
|
|||
| Univariate | Stepwise backward regression | Univariate | Stepwise backward regression | |
|
|
|
|||
| OR (95% CI) | Adjusted OR (95% CI) | OR (95% CI) | Adjusted OR (95% CI) | |
| More than six ribs | 0.79 (0.27–2.19) | 2.75 (0.76–10.04) | 3.19 (0.75–14.51) | |
|
|
||||
| Sex | 0.34 (0.07–1.21) | 0.35 (0.07–1.26) | 0.33 (0.02–1.94) | |
|
|
||||
| Age | 0.99 (0.95–1.03) | 0.94 (0.88–0.99) | 0.92 (0.86–0.98) | |
|
|
||||
| Associated thoracic injurya | 0.63 (0.29–1.22) | 0.83 (0.28–1.83) | ||
|
|
||||
| Flail chest | 0.50 (0.13–1.85) | 2.20 (0.36–42.49) | ||
|
|
||||
| Lung contusion | 0.52 (0.19–1.37) | 1.61 (0.45–5.73) | ||
|
|
||||
| Underlying lung disease | 0.62 (0.11–3.61) | 0.91 (0.13–18.39) | ||
|
|
||||
| Bilateral rib fractures | 0.37 (0.13–0.99) | 0.70 (0.20–2.62) | ||
- 1. Ziegler DW, Agarwal NN. The morbidity and mortality of rib fractures. J Trauma 1994;37:975–9.ArticlePubMed
- 2. Gabram SG, Schwartz RJ, Jacobs LM, Lawrence D, Murphy MA, Morrow JS, et al. Clinical management of blunt trauma patients unilateral rib fractures: a randomized trial. World J Surg 1995;19:388–93.ArticlePubMedPDF
- 3. Jones D, Nelson A, Ma OJ. Pulmonary trauma. In: Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM, editors. Tintinalli’s emegency medicine. 8th ed. New York: McGraw Hill; 2016. p. 1750–1.
- 4. Lee RB, Bass SM, Morris JA Jr, MacKenzie EJ. Three or more rib fractures as an indicator for transfer to a level I trauma center: a population-based study. J Trauma 1990;30:689–94.ArticlePubMed
- 5. Flagel BT, Luchette FA, Reed RL, Esposito TJ, Davis KA, Santaniello JM, et al. Half-a-dozen ribs: the breakpoint for mortality. Surgery 2005;138:717–23; discussion 723–5, ArticlePubMed
- 6. Barnea Y, Kashtan H, Skornick Y, Werbin N. Isolated rib fractures in elderly patients: mortality and morbidity. Can J Surg 2002;45:43–6.PubMedPMC
- 7. Sirmali M, Türüt H, Topçu S, Gülhan E, Yazici U, Kaya S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg 2003;24:133–8.ArticlePubMedPDF
- 8. May L, Hillermann C, Patil S. Rib fracture management. BJA Education 2015;16:26–32.ArticlePDF
- 9. Lucid WA, Taylor TB. Thoracic trauma. In: Strange GR, editor. Pediatric emergency medicine: a comprehensive study guide. New York: McGraw-Hill, Medical Publishing Division; 2002. p. 92–100.
- 10. Bastos R, Calhoon JH, Baisden CE. Flail chest and pulmonary contusion. Sem Thorac Cardiovasc Surg 2008;20:39–45.Article
- 11. Heck HA, Levitzky MG. The respiratory system. In: O’Leary JP, Tabuenca A, Capote LR, editors. The Physiologic basis of surgery. 4th ed. Hagerstown: Lippincott Williams & Wilkins; 2007. p. 463.
- 12. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. EurRespir J 2005;26:319–38.Article
- 13. Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F, et al. Standardisation of the measurement of lung volumes. EurRespir J 2005;26:511–22.Article
- 14. Bulger EM, Arneson MA, Mock CN, Jurkovich GJ. Rib fractures in elderly. J Trauma 2000;48:1040–6; discussion 1046–7, ArticlePubMed
- 15. Holcomb JB, McMullin NR, Kozar RA, Lygas MH, Moore FA. Morbidity from rib fractures increases after age 45. J Am CollSurg 2003;196:549–55. Article
- 16. Livingston DH, Richardson JD. Pulmonary disability after severe blunt chest trauma. J Trauma 1990;30:562–6; discussion 566–7, ArticlePubMed
- 17. Amital A, Shitrit D, Fox BD, Raviv Y, Fuks L, Terner I, et al. Long term pulmonary function after recovery from pulmonary contusion due to Blunt chest trauma. Isr Med Assoc J 2009;11:673–6. PubMed
- 18. Hwang JJ, Kim YJ, Ryu HY, Cho HM. Early surgical stabilization of ribs for severe multiple rib rractures. J Korean Soc Traumatol 2011;24:12–7.
- 19. Lardinois D, Krueger T, Dusmet M, Ghisletta N, Gugger M, Ris HB. Pulmonary function testing after operative stabilisation of the chest wall for flail chest. Eur J Cardiothorac Surg 2001;20:496–501.ArticlePubMedPDF
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Prevalence of chronic post-thoracotomy pain in patients with traumatic multiple rib fractures in South Korea: a cross-sectional study
Kun Hyung Kim, Chan Kyu Lee, Seon Hee Kim, Youngwoong Kim, Jung Eun Kim, Yu Kyung Shin, Junepill Seok, Hyun Min Cho
Scientific Reports.2021;[Epub] CrossRef - Yoga—An Alternative Form of Therapy in Patients with Blunt Chest Trauma: A Randomized Controlled Trial
Mallikarjun Gunjiganvi, Purva Mathur, Minu Kumari, Karan Madan, Atin Kumar, Rajesh Sagar, Sushma Sagar, Amit Gupta, Biplab Mishra, Altaf Hussain Mir, Mohini Meti, Subodh Kumar
World Journal of Surgery.2021; 45(7): 2015. CrossRef - Medicolegal Evaluation of Long-Term Respiratory Functions in Patients Injured Due to Traffic Accidents
Esra Dugral, Aydin Sanli, İsmail Ozgur Can
Cureus.2021;[Epub] CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

