Early Predictive Values for Severe Rhabdomyolysis in Blunt Trauma
Article information
Abstract
Purpose
Rhabdomyolysis (RB) is a syndrome characterized by the decomposition of striated muscles and leakage of their contents into the bloodstream. Acute kidney injury (AKI) is the most significant and serious complication of RB and is a major cause of mortality in patients with RB. Severe RB (creatine kinase [CK] ≥5,000) has been associated with AKI. However, early prediction is difficult because CK can reach peak levels 1–3 days after the trauma. Hence, the aim of our study was to identify predictors of severe RB using initial patient information and parameters.
Methods
We retrospectively analyzed 1,023 blunt trauma patients admitted to a single tertiary hospital between August 2011 and March 2018. Patients with previously diagnosed chronic kidney disease were excluded from the study. RB and severe RB were defined as a CK level ≥1,000 U/L and ≥5,000 U/L, respectively. The diagnosis of AKI was based on RIFLE criteria.
Results
The overall incidence of RB and severe RB was 31.3% (n=320) and 6.2% (n=63), respectively. On multivariable analysis, male sex (odds ratio [OR] 3.78, 95% confidence interval [CI] 1.43 to 10.00), initial base excess (OR 0.85, 95% CI 0.80 to 0.90), initial CK (OR 2.07, 95% CI 1.67 to 2.57), and extremity abbreviated injury scale score (OR 1.78, 95% CI 1.39 to 2.29) were found to predict severe RB. The results of receiver operating characteristic analysis showed that the best cutoff value for the initial serum CK level predictive of severe RB was 1,494 U/L.
Conclusions
Male patients with severe extremity injuries, low base excess, and initial CK level >1,500 U/L should receive vigorous fluid resuscitation.
INTRODUCTION
Rhabdomyolysis (RB) is a syndrome characterized by the decomposition of striated muscles and leakage of their contents into the bloodstream, including electrolytes, myoglobin, and other sarcoplasmic proteins (e.g., creatine kinase [CK], lactate dehydrogenase, alanine aminotransferase, and aspartate aminotransferase) [1]. The presentation of RB ranges from asymptomatic elevation of serum CK to life-threatening conditions such as acute kidney injury (AKI), cardiac arrhythmias, compartment syndrome, hypovolemic shock, and disseminated intravascular coagulation [1,2].
AKI is the most significant and serious complication of RB and major cause of mortality among RB patients [1]. Myoglobin plays a major role in the pathogenesis of RB-induced AKI. However, myoglobin is not an appropriate diagnostic marker. Because of its short half-life (2–3 hours), myoglobin is rapidly metabolized and excreted [3]. The most sensitive biomarker of muscle injury is the serum CK level. The diagnosis of RB is generally made when CK levels are five times the upper normal limit (>1,000 U/L) in the presence of skeletal muscle injury [4,5]. CK is not directly involved in the pathogenesis of myoglobinuric AKI, but CK levels >5.000 U/L indicate serious muscle injury and are associated with the onset of AKI and mortality [3,6].
The most common cause of RB is trauma accompanied by muscle damage [3,4,7]. Myoglobinuric AKI can be prevented with timely and vigorous fluid resuscitation. However, recent studies have shown that large volumes of fluid could worsen the outcome in view of coagulopathy and hypothermia [8]. Therefore, it is important to identify the group of trauma patients at high risk for AKI. Numerous studies have evaluated the risk factors for AKI in RB patients. Most have shown that the peak CK level is associated with AKI [2,6,9]. However, CK can reach peak levels 1–3 days after trauma [3]. Hence, the aim of our study was to identify predictors of severe RB on the basis of initial patient information and parameters.
METHODS
Patient enrollment and data collection
We conducted a retrospective observational study of blunt trauma patients admitted to a single tertiary hospital in Seoul, Korea between August 2011 and March 2018. We selected all subjects who had visited ER after trauma during our study period, and excluded them using following criteria: 1) patients who did not undergo blood CK level test, 2) no blunt trauma, 3) patients who discharged or transferred out at ER, 4) patients with known chronic kidney disease (CKD), 5) patients who transferred from another hospital in chronic phase, and 6) patients who died within first 48 hours after arriving to the ER. Data on patient ages, sex, injury severity score (ISS), and abbreviated injury scale (AIS) score were extracted from electronic files. Initial blood pressure, heart rate, pH, base excess (BE), lactate, and hemoglobin (Hb) values were analyzed at the time of presentation to the hospital. Peak CK levels were determined within 72 hours of trauma. Given that the diagnosis of RB is made when the CK levels are five times the upper normal limit (1,000 U/L), we considered 5,000 U/L as the cut-off in the diagnosis of severe RB [3,6]. Patients previously diagnosed with chronic kidney disease and those who died during the first 48 hours after presentation were excluded (Fig. 1).
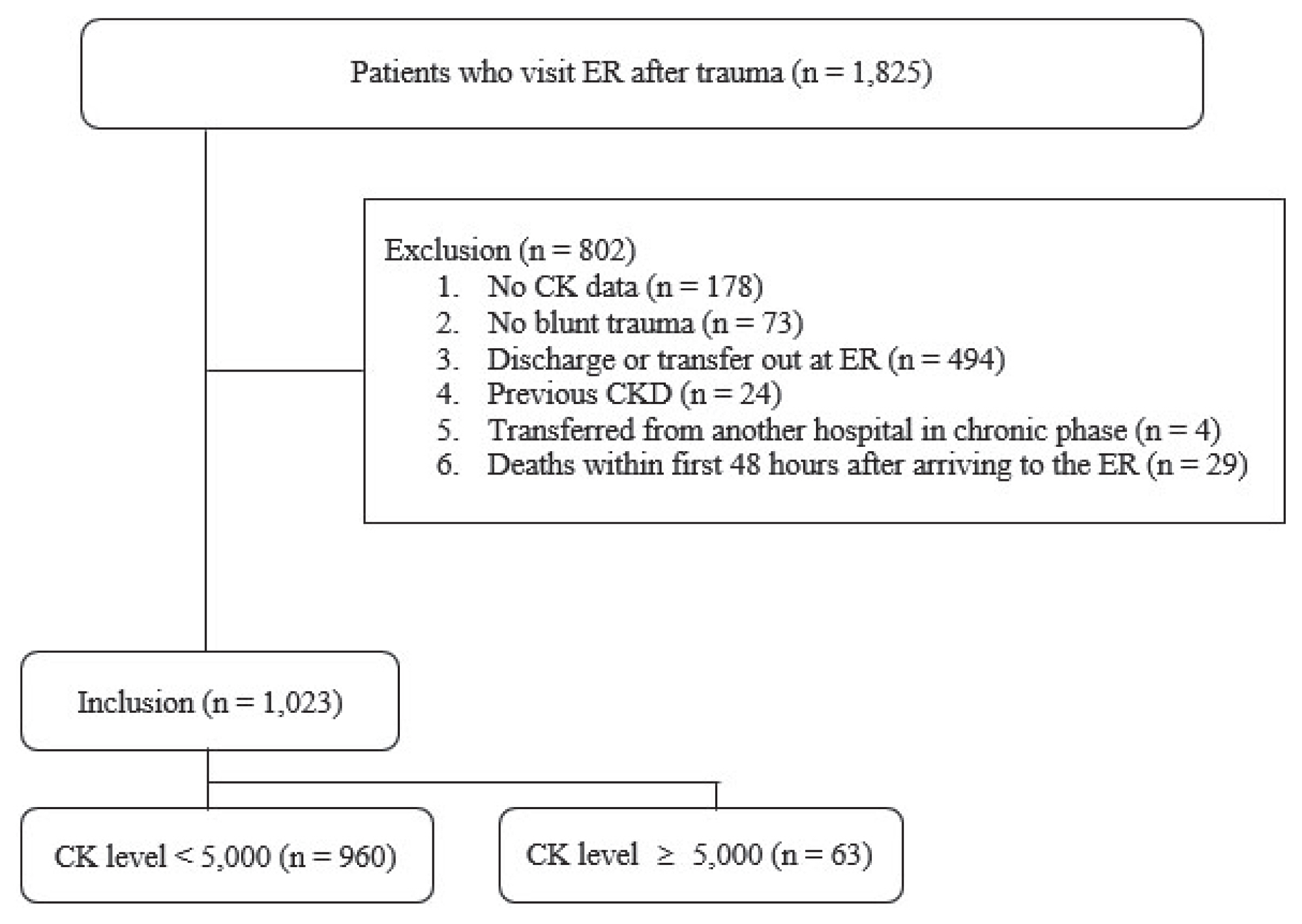
Flow diagram of article selection and the inclusion/exclusion process. ER: emergency room, CK: creatine kinase, CKD: chronic kidney disease.
Clinical variables
The acute dialysis quality initiative criteria (risk, injury, and failure, and loss, and end-stage kidney disease; RIFLE classification) were used to classify AKI. The RIFLE classification defines three grades of increasing severity of AKI, that is, risk (R), injury (I), and failure (F), as well as two outcome variables, that is, loss (L) and end-stage kidney disease (E) (Fig. 2) [10]. We calculated the baseline creatinine level of patients without CKD from the Modification of Diet in Renal Disease equation using an estimated glomerular filtration rate of 75 mL/min/1.73 m2, similar to previous studies [11]. For analysis, patients were assigned to their worst RIFLE category according to serum creatinine criteria during the first 7 days after admission.

Statistical analysis
Categorical variables were analyzed using the χ2 test or Fisher’s exact test, as appropriate. Continuous variables were analyzed using Student’s t-test. A p-value less than 0.05 was considered statistically significant. A multiple logistic regression model was then developed using the variables that were determined to be significantly associated with severe RB. Distributions of variables were reported as mean±standard deviation (SD) (percentages) and median (interquartile range). Receiver operating characteristic (ROC) analysis was used to evaluate the appropriate cutoff points of the biomarkers and to assess the sensitivity and specificity of the predictors for severe RB. The test characteristics of these different cutoff values, including sensitivity, specificity, and area under the ROC curve (AUC), were determined. Statistical analyses were performed with IBM SPSS software (version 23.0; IBM, Armonk, NY, USA).
RESULT
Initial clinical and laboratory variables
During the study period (August 2011 to March 2018), we analyzed 1,023 patients (729 males and 294 females; age, 47.7±19.6, mean±SD) admitted with blunt trauma, who met the criteria. Of 63 patients with severe RB, 30 (47.6%) developed AKI, 16 (25.4%) needed renal replacement therapy, and nine (14.3%) died within 30 hospital days (Table 1). Patients with severe RB were more likely to be male and to have a significantly lower systolic blood pressure. They were also noted to have higher ISS, especially extremity AIS scores. There was no difference in the head & neck AIS scores (2 [0–3] vs. 2 [0–3], p=0.822) (Table 2).
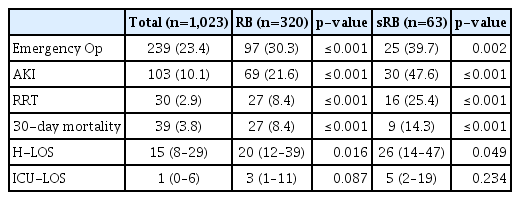
Outcomes according to RB and sRB

Characteristics according to sRB
When comparing initial laboratory values between the groups (with or without severe RB), indicators of metabolic acidosis, including pH, lactate, BE, and bicarbonate showed significant differences. CK, creatinine, and most ions, including Mg2+, K+, and P− were higher in the severe RB group, whereas Ca2+ and Hb were lower (Table 3).

Univariable analysis of initial laboratory values according to sRB
Multivariable logistic regression and ROC analysis of risk factors for severe RB
Using the variables that showed statistically significant results in Tables 2 and 3, multivariable logistic regression analysis was performed (Table 4). Male sex (odds ratio [OR] 3.78, 95% confidence interval [CI] 1.43 to 10.00), BE (OR 0.85, 95% CI 0.80 to 0.90), CK (OR 2.07, 95% CI 1.67 to 2.57), and extremity AIS scores (OR 1.78, 95% CI 1.39 to 2.29) were predictive of severe RB. As the CK range was very wide, 1/1,000 values were used for analysis. ROC analysis showed that the AUC for the initial serum CK level predictive of severe RB was 0.80 (Fig. 3) and that the best cutoff value for the initial serum CK level predictive of severe RB was 1,494 U/L (sensitivity, 0.46; specificity, 0.90).
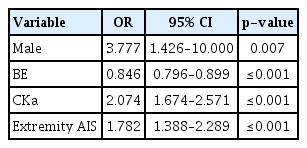
Multivariable logistic regression analysis of risk factors for sRB
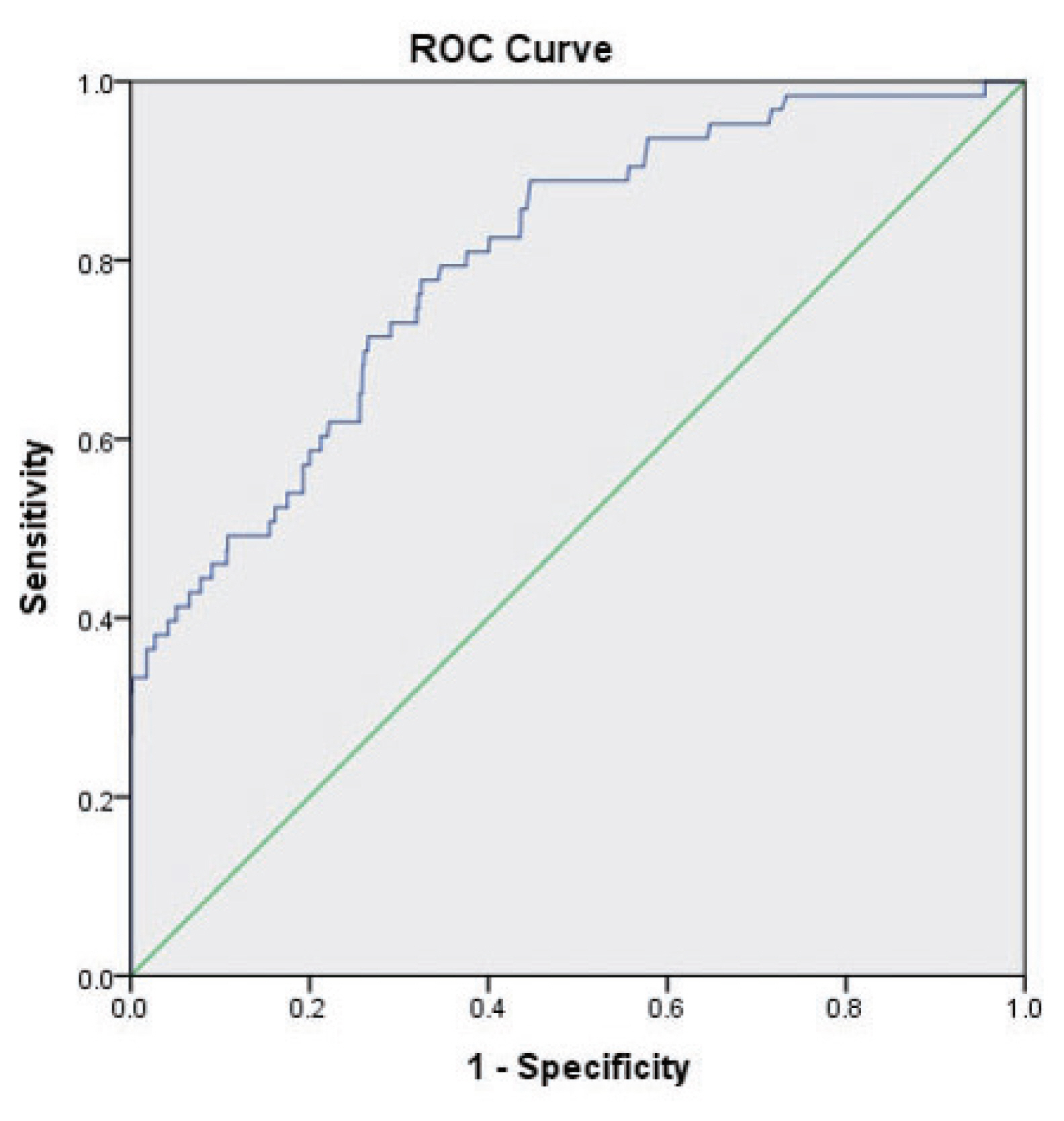
Receiver operating characteristic curve for initial serum creatine kinase in predicting severe rhabdomyolysis caused by blunt trauma. ROC: receiver operating characteristic.
DISCUSSION
The mortality rate of RB varies widely according to the study population, cause of RB, and diagnostic cutoff point for RB [1,3]. Veenstra et al. [12], in a study of 93 patients with severe RB, reported mortality of 32% and an AKI incidence of 51%. In this study, the 30-day mortality rate was significantly higher in the severe RB group, and the incidence of AKI was similar to that in the previous study. Safari et al. [6], in a recent meta-analysis that evaluated the relationship between serum CK and the development of RB-induced AKI, showed a significant association between the mean serum CK level and risk for AKI [6]. However, as cutoff points ranged from 1,000 to 15,000 U/L in prior studies, the hazardous cutoff point for CK in the development of AKI remains unclear. Furthermore, because the peak value develops during the hospital stay, the CK level presented in previous studies cannot be used to predict the risk of AKI in the early stage.
In this study, male sex, BE, CK level, and extremity AIS score were found to be early predictors of severe RB. In particular, the AUC for initial CK was considered to be “good” at predicting severe RB. The specificity is more important in setting the cutoff point for the CK level, as previous studies have suggested higher prophylactic volume infusions of up to 4–6 L per day. Therefore, we suggest 1,500 U/L (specificity >0.90) as the initial CK cutoff value for severe RB.
Several limitations of the present study should be considered. The results were based on a retrospective, single-center review of medical records. Of the 1,023 patients, only 63 patients met criteria for severe RB, and it is relatively small sample size. Details of the trauma mechanism may not have been rigorously documented, and not all serologic tests were performed in all patients. In addition, the basal creatinine level was calculated as a glomerular filtration rate of 0.75 for all patients without CKD because the basal creatinine level was unknown in the majority of patients. Consequently, the actual incidence of AKI might be different. These limitations may lead to some bias in analyzing the factors associated with severe RB and AKI.
CONCLUSION
AKI is the most significant and serious complication of RB and major cause of mortality among RB patients. Severe RB has been strongly associated with the onset of AKI and mortality. Male sex, initial BE, initial serum levels of CK, and extremity AIS score can be key predictors of severe RB that can lead to AKI. We suggest that male patients with severe extremity injury, low BE, and initial CK level >1,500 U/L should receive vigorous fluid resuscitation.