Misinterpretation of a skin fold artifact as pneumothorax on the chest x-ray of a trauma patient in Korea: a case report
Article information

Abstract
Misinterpreting radiographic findings can lead to unnecessary interventions and potential patient harm. The urgency required when responding to the compromised health of trauma patients can increase the likelihood of misinterpreting chest x-rays in critical situations. We present the case report of a trauma patient whose skin fold artifacts were mistaken for pneumothorax on a follow-up chest x-ray, resulting in unnecessary chest tube insertion. We hope to help others differentiate between skin folds and pneumothorax on the chest x-rays of trauma patients by considering factors such as location, shape, sharpness, and vascular markings.
INTRODUCTION
Chest x-ray (CXR) is the most readily available and common imaging modality for trauma patients, providing information on the patient's overall thoracic health and helping to identify thoracic injuries [1]. However, the interpretation of CXRs can be challenging, particularly when adequate image quality is difficult to obtain in a seriously injured patient [2]. The likelihood of image artifact and misinterpretation of the CXR increases when the patient has multiple monitoring and resuscitation lines and devices in the chest [3]. According to previous reports, approximately 10% of errors occurred during interpretation of the CXR, as the interpretation of CXRs is subject to human error and depends on reader expertise [4].
A skin fold artifact is one of the commonly encountered artifacts on CXR that can mimic pneumothorax [5]. Failure to differentiate between true pneumothorax and a skin fold artifact can lead to unnecessary interventions and complications, such as iatrogenic bleeding, prolonged hospital stays, and increased healthcare costs [6].
CASE REPORT
A 72-year-old man presented to the emergency department with injuries from a fall. The initial assessment showed multiple bilateral rib and spine fractures as well as pelvic bone fractures. The initial chest computed tomography and CXR (Fig. 1) showed bilateral hemothorax, so chest tubes were inserted (not shown here). After 6 days of hospitalization, the right chest tube was removed due to decreased hemothorax (Fig. 2A). However, after 8 days of hospitalization, acute pneumothorax was suspected (Fig. 2B) on the follow-up CXR, prompting bedside chest tube reinsertion (Fig. 2C). As there was no evidence of air drainage from the chest tube and a repeat CXR the next day showed no pneumothorax, interdepartment consultation was requested with radiology. The thoracic radiologists confirmed that it was a skin fold and not an actual pneumothorax, leading to removal of the chest tube. The follow-up CXR (Fig. 2D) again showed multiple skin folds from a different view.
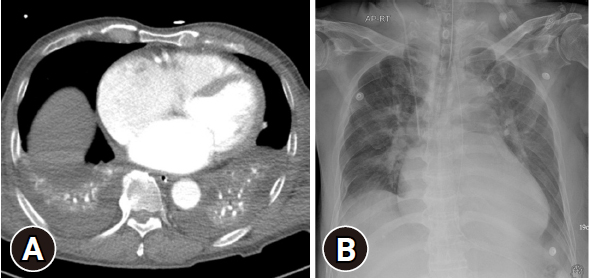
Initial images show bilateral hemothorax. (A) Chest computed tomography. (B) Chest x-ray.
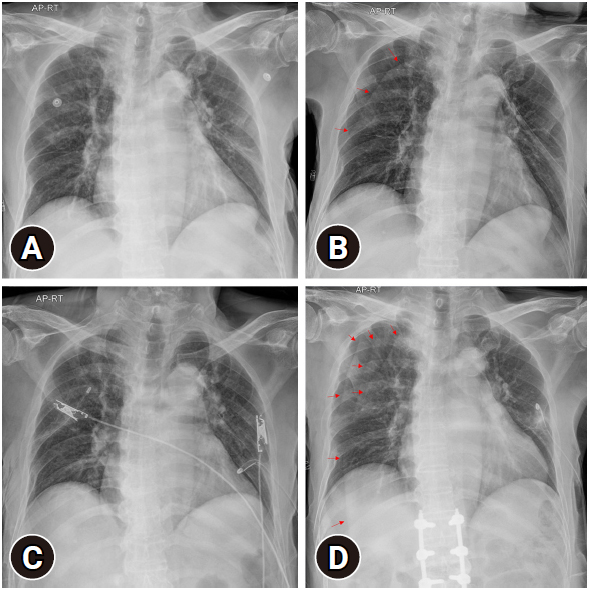
Chest x-ray (CXR) images after hospitalization. (A) After 6 days of hospitalization, CXR shows removal of the right chest tube. (B) After 8 days of hospitalization, CXR shows the right-side skin fold (arrows), which was misdiagnosed as new pneumothorax. (C) To treat the apparent pneumothorax, a chest tube was immediately reinserted at the bedside. (D) The subsequent follow-up CXR after 10 days of hospitalization reveals multiple curvilinear lines (arrows) extending to the upper abdomen on the right, representing skin folds.
Ethics statement
This study was approved by the Institutional Review Board of Gachon University College of Medicine (No. GAIRB2023-216), which waived the requirement for informed consent.
DISCUSSION
Chest radiography is a common diagnostic test used to evaluate chest pathologies such as pneumothorax, hemothorax, pneumonia, and lung injury in injured patients since it allows easy and fast assessment [7,8]. However, normal structures such as nipples and skin folds and clothing items like buttons or attached electrocardiography leads can be misinterpreted as abnormal findings on CXR [9–11]. Skin fold artifacts are commonly encountered on CXRs, especially in patients with obesity or those unable to cooperate with optimal positioning during the examination [12,13]. These artifacts can mimic various pathological conditions, including pneumothorax, leading to potential misdiagnosis and unnecessary interventions. Therefore, clinicians must be able to recognize these artifacts and pay special attention when interpreting the CXRs of traumatized patients.
Some tips for differentiating pneumothorax from a skin fold on CXR include the following [14,15]:
1. Location: Pneumothorax typically appears along the lung periphery, whereas a skin fold commonly appears to continue beyond the chest wall.
2. Shape and sharpness: The linear shadow of pneumothorax tends to be thin, sharp, and well-defined. A skin fold usually appears wider and ill-defined towards the medial side, while appearing sharp towards the lateral side.
3. Vascular markings: The distal portion of the linear shadow of pneumothorax often lacks visible pulmonary vessels, whereas the distal portion of a skin fold may still demonstrate pulmonary vessel markings.
In situations where pneumothorax and skin fold can be easily confused, clinicians should consider these radiological tips when making decisions, while also taking into account the clinical context and other relevant factors.
Notes
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
This study was supported by a grant from Gachon University Gil Medical Center (No. FRD2021-11).
Author contributions
Conceptualization: EYK; Funding acquisition: EYK; Methodology: YP; Visualization: YP; Writing–original draft: YP; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.