Traumatic tension enterothorax in New Zealand: a case report
Article information

Abstract
Traumatic rupture of the right hemidiaphragm occurred following a high-velocity motor vehicle collision in the case presented herein. The resulting herniation of small bowel loops into the thorax resulted in hemodynamic and respiratory compromise due to pressure effects on the right heart and major vessels. The patient’s hemodynamic status improved with reduction of enterothorax, and the diaphragmatic defect was repaired. We discuss the available literature and learning points from this rare case.
INTRODUCTION
A 59-year-old man was involved in a high-speed motor vehicle collision as a restrained driver. On retrieval by paramedics the patient was in respiratory distress with a Glasgow Coma Scale score of 7; therefore, he was intubated at the scene. Due to absent breath sounds on the right side, there was a concern for a right-sided hemopneumothorax. Needle decompression was performed, followed by an intercostal chest drain with minimal bloody output.
CASE REPORT
On arrival at the emergency department, the patient was hypotensive and tachycardic with an unstable anteroposterior compression fracture of the pelvis on X-ray (Fig. 1). A chest X-ray was interpreted as being consistent with pulmonary contusion (Fig. 2) and a focused assessment with sonography for trauma scan was negative. Therefore, whilst being resuscitated with blood products, the patient was taken to the hybrid operating room for iliac angiography, which demonstrated proximal cutoff of the left and right internal iliac arteries. These were both embolized, followed by a temporary improvement in the patient’s hemodynamic status. Following this, the patient proceeded to a computed tomography (CT) trauma scan, which revealed a traumatic right diaphragmatic rupture with almost the entire small bowel herniating into the right hemithorax with mediastinal shift and compression of the right heart chambers and inferior vena cava (Fig. 3). The patient deteriorated from a hemodynamic standpoint during the CT scan and was taken to the operating room for a trauma laparotomy where the small bowel loops were reduced by gentle traction into the abdomen until complete. A 10-cm diaphragmatic defect was found anterior to the liver (Fig. 4). Access to the defect required ligation and division of the falciform ligament, and the defect was repaired using a running 0-Ethibond suture (Ethicon Inc). The patient’s hemodynamic status improved markedly following reduction of enterothorax.
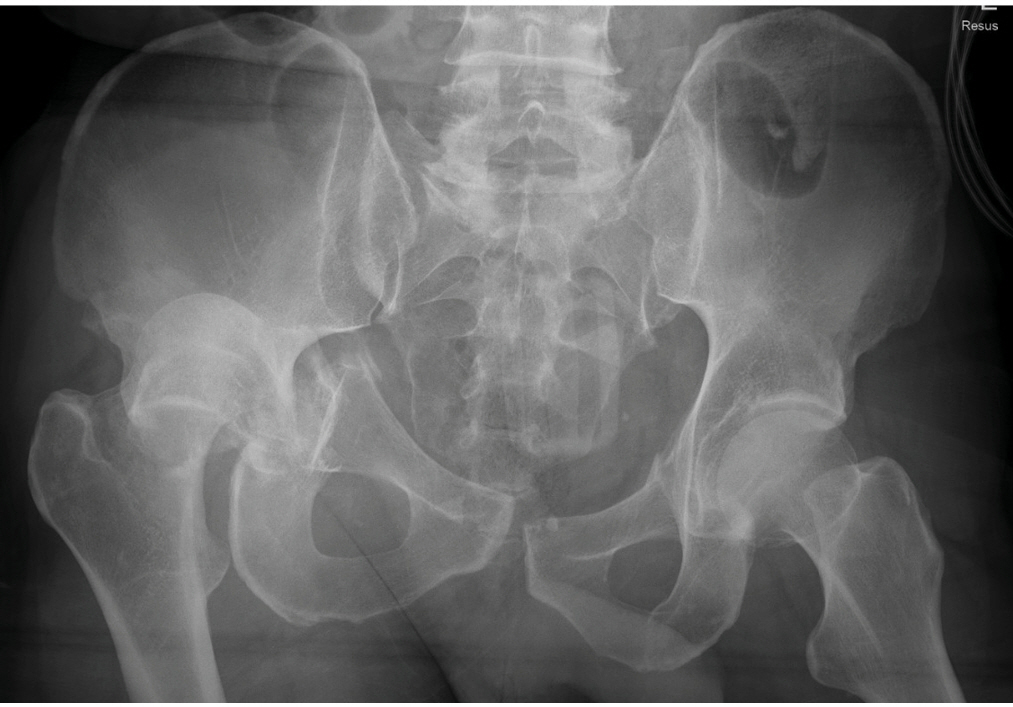
Pelvic X-ray demonstrating an unstable pelvic fracture.
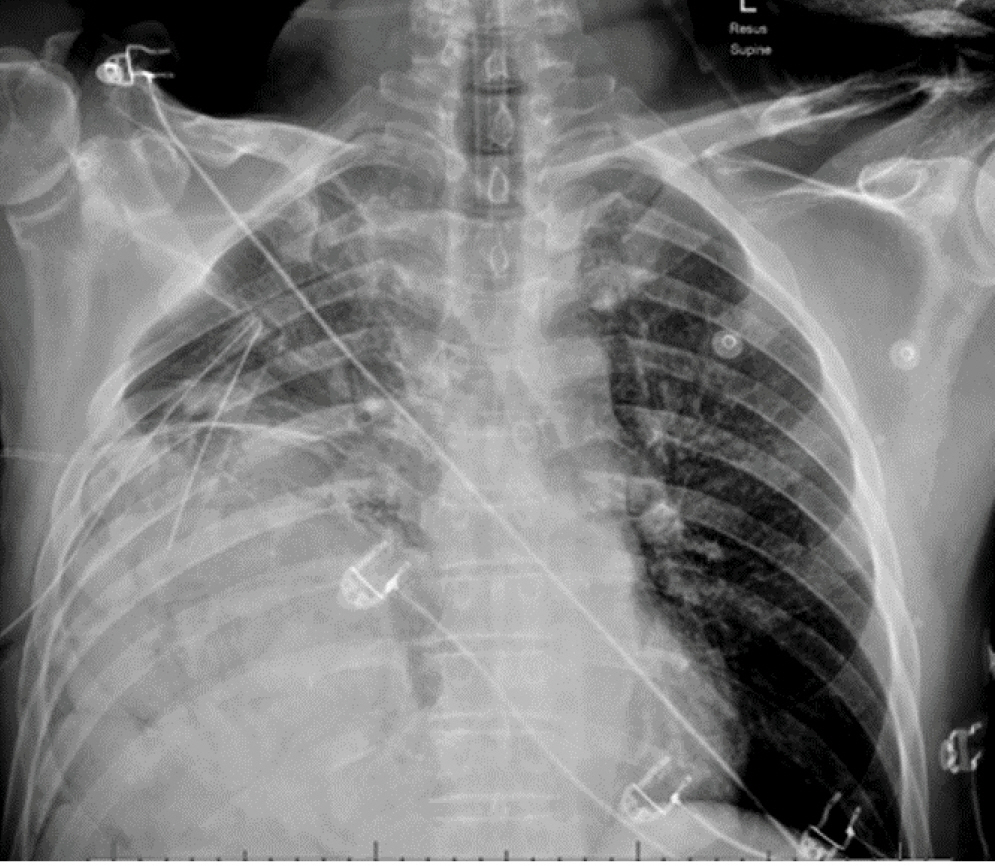
Chest X-ray on arrival at the emergency department.
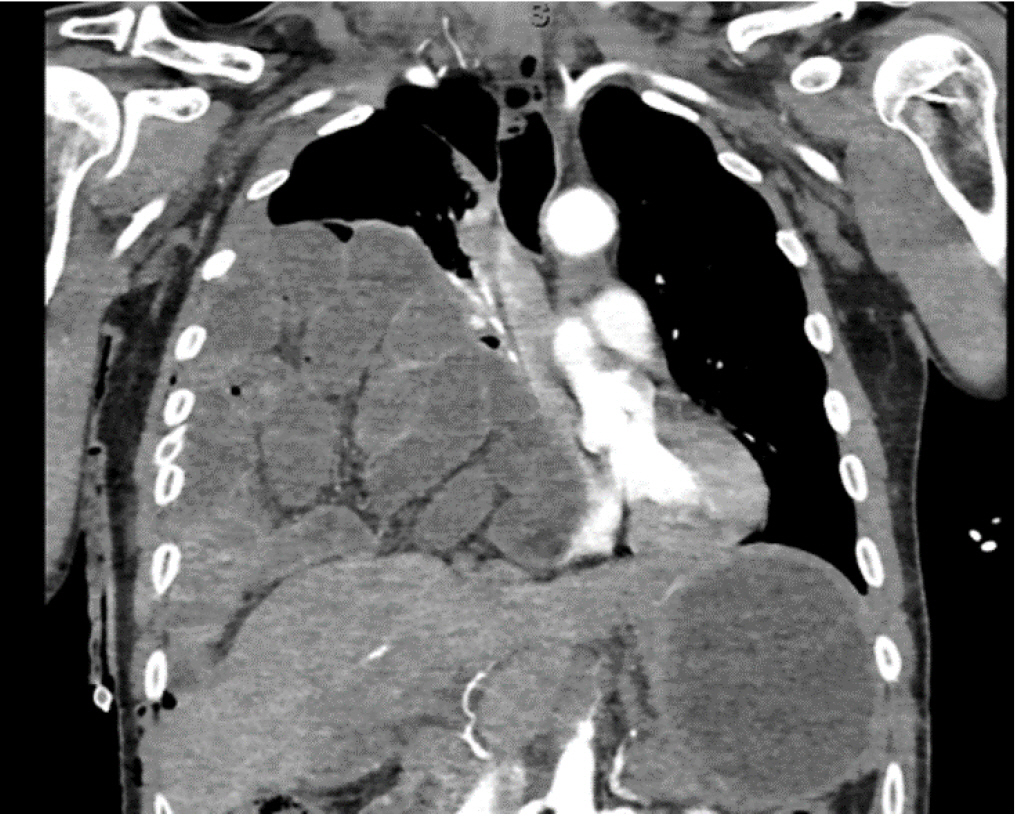
Coronal slice of chest and abdominal computed tomography showing enterothorax.
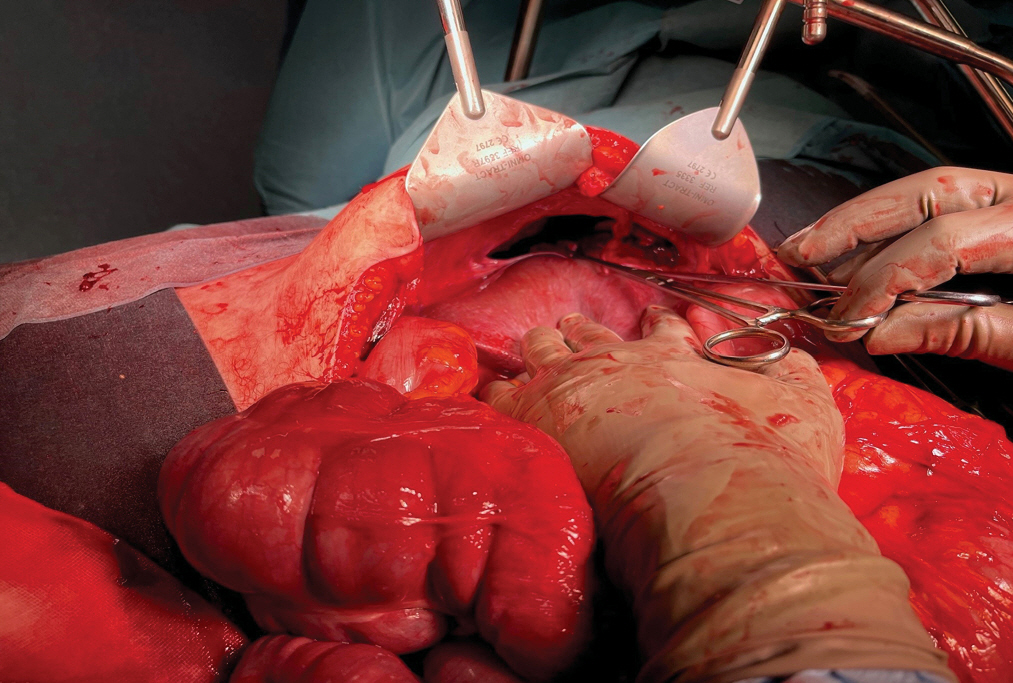
Intraoperative photograph of the diaphragmatic defect.
Ethics statement
The patient provided informed consent for publication of the research details and clinical images.
DISCUSSION
Traumatic diaphragmatic ruptures occur in only 1% to 7% of major blunt trauma patients but are found more frequently in cases of penetrating trauma (10%–15%). On the right side, the liver typically provides a protective effect due to its mass effect, resulting in only a 19% incidence of herniation, in comparison to 58% of left diaphragmatic ruptures [1].
Tension enterothorax is extremely rare, with only a small number of case reports in the published literature [1–4]. In addition to trauma, instances of postoperative enterothorax have been reported, such as following Ivor Lewis esophagectomy [4]. We propose that the pathophysiology of tension enterothorax involves the small bowel becoming obstructed at the diaphragmatic defect and then going on to distend and occupy increasing space within the thoracic cavity. This then impedes venous return through a pressure effect on the major vessels and right heart, as occurs in tension pneumothorax.
There are a number of important learning points to take from the case we describe. An intercostal chest drain was inserted for suspected hemopneumothorax. Clearly, intercostal chest drain insertion in a patient with enterothorax could have caused significant harm. Subsequent to this, a chest X-ray was misinterpreted as showing pulmonary contusion. Had enterothorax been recognized at this stage, the patient would have proceeded directly to laparotomy. Instead, the patient’s hemodynamic status was attributed to bleeding from an unstable pelvic fracture. Awareness of enterothorax in the differential diagnosis for respiratory distress following blunt abdominal trauma is important for avoiding potential harm.
In conclusion, although a rare phenomenon, diaphragmatic rupture with enterothorax must be considered in the differential diagnosis of patients with respiratory distress following blunt abdominal trauma.
Notes
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
The authors did not receive any financial support for this study.
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.
Author contributions
Conceptualization: AG, DAY; Data curation: MM, AG; Formal analysis: NA; Writing–original draft: MM, AG; Writing–review & editing: all authors. All authors read and approved the final manuscript.