Ruptured uterus in a 36-week pregnant patient with hemorrhagic shock after blunt trauma in Korea: a case report
Article information

Abstract
Traumatic uterine rupture is uncommon but can be fatal and life-threatening for both the mother and infant. In addition to complications caused by trauma itself, such as pelvic fracture, gestational complications such as placental abruption, abortion, premature labor, rupture of membranes, maternal death, and stillbirth can occur. In particular, fetuses have been reported to have a high mortality rate in cases of traumatic uterine rupture. A 35-year-old pregnant female patient fell from the fourth floor and was admitted to our trauma center. We observed large hemoperitoneum, pelvic fractures, and spleen laceration, and the fetus was presumed to be located outside the uterus. The pregnant woman was hemodynamically unstable. Although the fetus was stillborn, angioembolization and surgical treatment were properly performed through collaboration with an interventional radiologist, obstetrician, and trauma surgeons. After two orthopedic operations, the patient was discharged after 34 days. This case report suggests the importance of a multidisciplinary approach in the treatment of pregnant trauma patients.
INTRODUCTION
Traumatic injuries in pregnancy are not uncommon, accounting for 6%-7% of all traumatic injuries [1]. Even if the trauma is not serious, pregnant trauma patients are important because traumatic injuries during pregnancy are associated with abortion, premature labor, rupture of membrane, maternal death, and stillbirth [2]. Serious trauma in a pregnant woman is dangerous for both the mother and the fetus. The treatment priority of pregnant women is the same as the priority of severe trauma patients. However, it is difficult to determine the treatment plan for pregnant trauma patients due to the need to consider both the pregnant woman and the fetus. Furthermore, changes in maternal physiology and gestational age during trauma complicate an accurate evaluation of fetal outcomes [3].
In this case report, we describe a case of traumatic uterine rupture accompanied by a 36-week-old stillborn fetus removed from the abdominal cavity.
CASE REPORT
A 35-year-old female patient at 36 weeks' gestation was transferred from an outside hospital to Gachon University Gil Medical Center (Incheon, Korea) after falling from the fourth floor. Our trauma team was provided with the pregnant woman’s information from an outside hospital. The patient had been taking medication for bipolar disorder and voluntarily stopped taking the medication 3 days previously for breastfeeding. Emergency obstetrical ultrasound was performed on the patient at the outside hospital, and we were informed that the fetus was likely to be stillborn. The patient was hemodynamically unstable even before she left the hospital. She received transfusions of 7 units of red blood cells (RBCs) and 3 units of fresh frozen plasma (FFP) from the outside hospital. Five hours elapsed between the fall and the patient’s presentation to our trauma center.
When she arrived at our trauma center, the initial vital signs included a blood pressure of 90/76 mmHg and a heart rate of 144 beats/min. Since we had been notified of the stillbirth of the fetus based on obstetric ultrasonography conducted at the outside hospital, we performed an initial computed tomography (CT) scan during an emergency transfusion. The CT scan showed a large amount of hemoperitoneum, pelvic fracture, and spleen injury. A coronal image of contrast-enhanced abdominopelvic CT showed a disrupted wall of the uterine fundus and the fetus located in the peritoneal cavity, outside the uterus (Fig. 1).
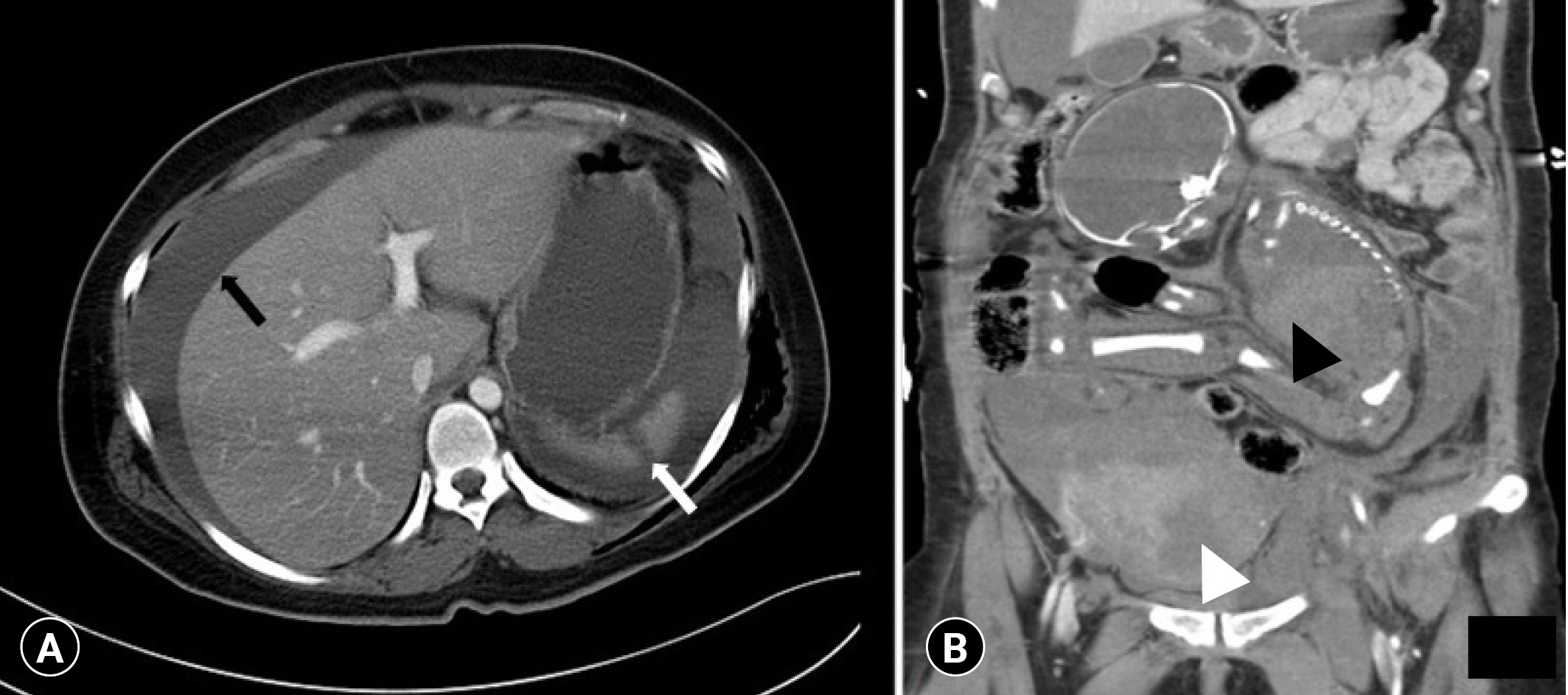
Computed tomography. (A) An axial view shows hemoperitoneum (black arrow) and spleen laceration (white arrow). (B) A coronal view shows the fetus (black arrowhead) located in the peritoneal cavity and the disrupted wall of uterine fundus (white arrowhead).
Before the patient arrived at our trauma center, we contacted an interventional radiologist and obstetrician in advance. Since a ruptured uterus causes massive bleeding, we decided to perform angioembolization first to reduce bleeding during surgery. As soon as the patient arrived in the emergency room, we performed an emergency blood transfusion for resuscitation. After resuscitation, we transferred the patient to the angiography room. Angiography confirmed that the contrast agent had leaked from both internal iliac artery and splenic artery. Bilateral iliac arteriography revealed mild hypertrophy of the bilateral uterine arteries, which were embolized using gelatin sponge particles for the right uterine artery and N-butyl-cyanoacrylate for the left uterine artery. (Fig. 2) The superior polar splenic arteries were also embolized with gelatin sponge particles. An interventional radiologist succeeded in embolizing a damaged artery. During angioembolization, the obstetrician and trauma surgeon were on standby for immediate surgery. After angioembolization, the patient was sent to the operating room.
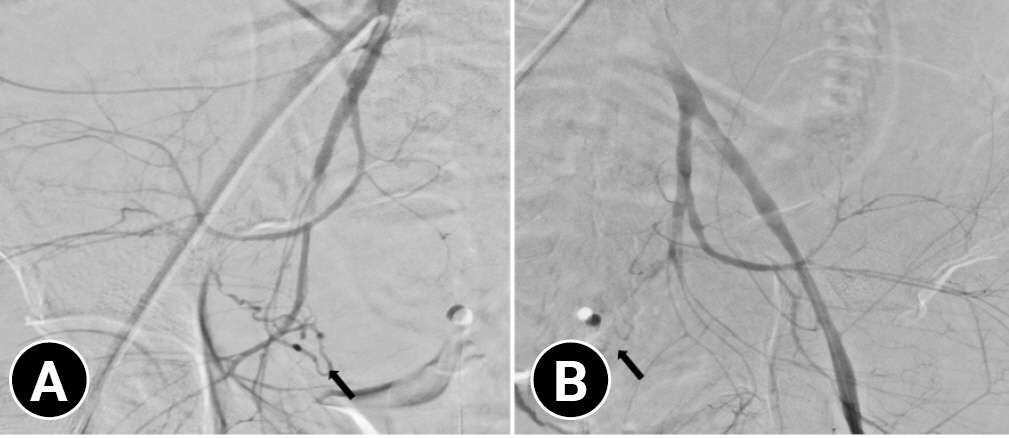
Bilateral iliac arteriography reveals mild hypertrophy of the bilateral uterine arteries (arrows), which were embolized using (A) gelatin sponge particles for the right uterine artery and (B) N-butyl-cyanoacrylate for the left uterine artery.
We consulted with an obstetrician so that the trauma surgeon and the obstetrician could operate together at the same time. First, the trauma surgeon opened the abdomen and performed gauze packing in the four quadrants of the abdominal cavity. Approximately 2,000 mL of hematoma was present in the abdominal cavity. At the same time, a stillborn fetus emerged from the ruptured uterus and was found in the intraabdominal free space (Fig. 3). The obstetrician cut the umbilical cord of the fetus and evacuated the fetus first. We then found a uterine rupture and the placenta attached to it. We isolated the placenta from the uterus, and obstetrician sutured the ruptured uterus with Vicryl 2-0 using a continuous running method (Fig. 4). Finally, the trauma surgeon operated for additional accompanying injuries, including cecal serosa tearing. There was no active bleeding other than hematoma in the lower quadrant of the retroperitoneum and a contusion of the stomach's great curvature. After removing the packing gauze from the four quadrants, the operation was terminated as the abdominal wound was temporarily closed. From hospitalization to our trauma center to the termination of laparotomy, she received six additional packs of RBCs and six additional packs of FFP. A second-look operation was performed for definite abdominal closure 2 days after the first operation.
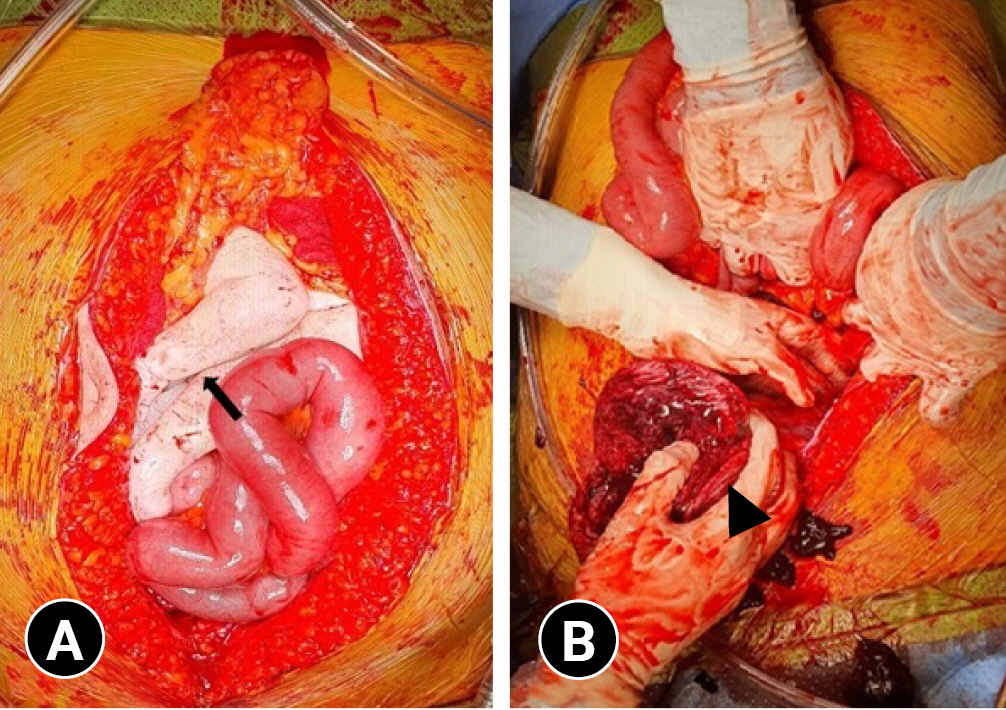
Images showing (A) the stillborn fetus located in the abdominal cavity outside the uterus (arrow) and (B) the ruptured uterus (arrowhead).

Images showing (A) the uterus repaired by an obstetrician and (B) the placenta separated from the pregnant woman.
The patient then underwent two orthopedic operations for a fracture of the left pelvic bone and a fracture of the right lateral tibial plateau during hospitalization. We consulted a psychiatrist in order for the patient to resume the psychiatric medication she had stopped for lactation. The patient was treated in the intensive care unit for 2 weeks and was discharged after 34 days of hospitalization.
Ethics statements
Informed consent for publication of the research details and clinical images was obtained from the patient.
DISCUSSION
In pregnant women, blunt trauma is the most common mechanism of injury [4]. Motor vehicle crashes are the leading cause of trauma in pregnant women, followed by falls [5].
Pregnancy causes anatomical and physiological changes. In the first trimester of pregnancy, the fetus is protected by the pelvis. At 20 weeks of gestation, the uterus is palpable at the umbilical level. At 36 weeks of gestation, the uterus enlarges, and the uterine wall becomes thinner, making it more vulnerable to trauma [6]. In pregnant women, tachycardia and hypotension may not develop until significant blood loss has occurred, which may delay the diagnosis of shock [7]. Hemorrhage during pregnancy can significantly decrease blood flow to the uterus [7]. These changes affect the patient’s symptoms, laboratory findings, and radiologic imaging finding, which makes it difficult for trauma surgeons to decide on the treatment plan.
The mechanism of injury may be direct trauma to abdomen or indirect trauma due to deceleration or a shearing force. Direct fetal trauma accounts for fewer than 1% of cases of severe abdominal trauma in pregnant women, but fetal deaths are reported in 3.7% to 17.5% of those cases [8,9]. The risk of fetal loss correlates with the severity of the trauma and the maternal condition. In particular, it has been reported that the risk is higher in patients with an Injury Severity Score (ISS) >9 [3]. Although uterine rupture is rare, occurring in fewer than 1% of traumatic events during pregnancy, fetal mortality can reach 100% when traumatic uterine rupture occurs. In our case, the ISS of the patient was 50 and the uterus was ruptured [10]. Therefore, the risk of fetal mortality was expected to be very high.
Emergency treatment at the prehospital stage is important, and transfer to an appropriate trauma center is necessary. In our case, the patient was initially admitted to another hospital and appropriate resuscitation was not performed. When the patient presented to our trauma center, she was already in very severe shock. The initial evaluation of patients with pregnancy trauma should follow the Advanced Trauma Life Support algorithm, the same as the initial evaluation of nonpregnant trauma patients. In the early stages of hemorrhagic shock, isotonic crystalloids and massive transfusions should be considered. However, vasopressors should be considered last to support maternal blood pressure because they reduce uterine blood flow, which can lead to fetal hypoxemia [11].
Traumatic uterine ruptures are uncommon and difficult to diagnose. Furthermore, traumatic uterine rupture is dangerous for both the mother and fetus. Therefore, various specialties should be involved in caring for pregnant trauma patients, and a multidisciplinary treatment approach is very important. Caring for pregnant trauma patients requires an organized and integrated approach with an emergency medicine doctor or trauma surgeon as a team leader. A multidisciplinary treatment approach can reduce maternal-fetal morbidity and mortality, and in some cases, both the mother's life and the fetus can be preserved. Additionally, every trauma center that cares for these patients should have a protocol to ensure a standardized approach.
Notes
Author contributions
Conceptualization: JC, SJ, SP; Data curation: SJ; Formal analysis: SJ; Methodology: all authors; Project administration: JC; Visualization: all authors; Writing–original draft: SJ; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Conflicts of interest
Jayun Cho serves on the Editorial Board of Journal of Trauma and Injury, but was not involved in the peer reviewer selection, evaluation, or decision process of this article. The authors have no other conflicts of interest to declare.
Funding
The authors did not receive any financial support for this study.
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.
Additional information
This study was presented at the 9th Pan-Pacific Trauma Congress on June 2022 in Gyeongju, Korea.