The clinical pattern of intentional injuries at a primary Saudi Arabian trauma center
Article information

Abstract
Purpose
The term “intentional injuries” refers to a spectrum of injuries resulting from self-inflicted injuries, interpersonal violence, and group acts of violence. Intentional injuries are underreported in Saudi Arabia. This study aimed to analyze and evaluate the characteristics of intentional injuries in patients who presented to the emergency department of a primary trauma center in Medina, Saudi Arabia in 2013.
Methods
A prospective cohort database analysis of the clinical patterns and treatment outcomes of 252 patients who had intentional injuries between January and December 2013 was done.
Results
The proportion of trauma patients with intentional injuries was 1.3%. The mean age was 34.2±9.4 years, 141 patients (56.0%) were male, and 111 (44.1%) were female (male to female ratio, 1.27:1). The majority (n=159, 63.1%) of injuries occurred at night. Most occurred outside the home (n=180, 71.0%). Financial problems (n=62, 24.6%) and social disputes (n=61, 24.2%) were the most common reasons. Sharp objects (n=93, 36.9%) were the most common weapons used. The head and neck were the most commonly injured areas (n=63, 54.4%). Superficial cuts (n=87, 34.5%), were the most common type of injury. Suturing of wounds (n=54, 21.4%) and surgical debridement (n=47, 18.7%) were the most commonly performed modalities of management.
Conclusions
We conclude that intentional injuries in Saudi Arabia are a health care hazard that is, unfortunately, underreported. The clinical pattern is similar in most aspects to international reports but differs in certain features due to the specific religious and conservative characteristics of the community. Nationwide clinical studies are strongly recommended.
INTRODUCTION
An injury is defined as damage to the human body resulting from unintentional or intentional exposure to an energy source (mechanical, thermal, electrical, chemical, or radiant). Another definition is the state of insufficiency of vital elements (heat, oxygen) that exceeds the threshold of physiological tolerance, resulting in impairment or destruction of health. Both intentional and unintentional injuries have become a global public health concern regarding morbidity and mortality [1].
Injuries are one of the leading causes of death and disability throughout the world in all age groups under 60 years and are estimated to cause 10% to 30% of all hospital admissions across the globe and to account for approximately 9.6% of all deaths and 16% of all disabilities, with the greatest impact in developing countries [1,2]. Approximately five million people worldwide died as a result of an injury in 2010, accounting for nearly one in every 10 deaths. Of these, more than one in four were caused by an intentional injury [2].
Intentional injuries include interpersonal violence, child maltreatment, self-inflicted harm (burn, cut, bruises), community violence, or group-instigated acts of violence, homicide, sexual abuse, and suicide. Unintentional injuries include road traffic incidents, motor vehicle-related injuries, falls, drowning, environmental injuries, sports, and recreational injuries, poisoning, and fire-related injuries/burns [1,2].
In 2002, global data on the burden of injury showed that intentional injuries accounted for 1.5% of the disability-adjusted life years (DALYs) for 5- to 14-year-old girls and 2% of boys in this age group. In a panel of adolescents and young adults (15–29 years), the representation of intentional injuries among the total DALYs was slightly lower in female patients (1.2%), but dramatically higher in male patients (8.9%) [3]. While mortality represents a significant component of this impact, it is estimated that there are 20 to 40 victims of nonfatal violence for every death [4].
Intentional injuries form a spectrum (including self-inflicted injuries, interpersonal violence, and group acts of violence) of injuries caused by purposeful human action, whether directed at oneself or others. Intentional injuries include self-inflicted and interpersonal acts of violence intended to cause harm. They are very common and contribute significantly to morbidity and mortality and are reported to cause about nine deaths for every 100,000 persons, most of whom are economically productive individuals in the age range of 15 to 45 years. The reported significant risk factors for intentional injuries from interpersonal or self-inflicted violence include access to firearms, history of interpersonal violence, history of alcohol and drug abuse, mental illness, and poverty [5].
National, regional, cultural, and religious characteristics could influence the risk of intentional injuries, but the environmental factors that lead to injuries are often associated with other environmental health hazards. The diagnosis and recording of intentional injuries are problematic because intent could be difficult to assess, which led the World Health Organization to highlight two important points. The first is that the use of force does not necessarily correlate with the intent to damage. The second is that there may be differences in the intent to injure and the intent to use forms of violence that might be culturally acceptable in some settings [6].
Intentional injuries, which have been reported to represent a generally neglected, but growing epidemic in many developing countries, contribute substantially to the global injury burden, constitute a threat to the physical and psychological state of well-being of the victims, and are associated with substantial emotional and financial burdens on the community, family, and hospital resources [7]. The problem was found to be increasing at a fast rate in developing countries due to increasing conflicts over limited resources, unemployment, easy access to firearms, drug/alcohol abuse, substance misuse, and increased crime rates [8].
The socioeconomic impact of intentional injuries has received considerable attention due to the loss of productive years and the exhaustion of limited health care funds. Scientific studies and official reports have shown that the victims of intentional injuries constitute a socially and economically disadvantaged population because their medical care is poorly funded [9].
The 2010 Global Burden of Disease study indicated that intentional self-inflicted injuries rose by 23.8% between 1990 and 2010 in all ages [10]. Several studies in Saudi Arabia have documented the incidence and etiology of unintentional injuries, and trauma in general, using surveillance data, but no study has yet described the incidence, features, or outcomes of intentional injuries. There is a paucity of sufficient information in most developing countries regarding the morbidity and mortality of intentional injuries, as more concerns have been focused on the more common injuries related to road traffic and motor vehicle accidents at the expense of the less common category of self-inflicted injuries [11–14].
The purpose of this study was to evaluate and analyze the characteristics of intentional injuries in patients who presented to the emergency department of Al Ansar General Hospital, a primary trauma center in Medina, Saudi Arabia (ranked number 1 emergency center nationwide receiving emergency cases through 2012–2014), and to document the clinical patterns and outcomes of these intentional injuries.
METHODS
Ethical approval was granted from the Ethical Committee of Al Ansar General Hospital, Medina, Saudi Arabia and the management guidelines and clinical pathway subcommittee of the quality care program at the same hospital. A prospective cohort database analysis was conducted of the clinical patterns and treatment outcomes of Saudi Arabian patients involved in intentional injuries during the 12-month period between January and December 2013. Informed consent was obtained from all individual participants included in this study. The study protocol was designed using a digital database file in the outpatient department as part of the quality care program at Al Ansar General Hospital, Medina, Saudi Arabia.
All patients presented to the emergency department of the public health general hospital in Medina, Saudi Arabia. They were managed according to the Advanced Trauma Life Support protocol. The assessment of injuries, initial resuscitation, diagnostic workup, medical and supportive management, surgical procedures, and follow-up were carried out by the same surgical team with the participation of the emergency department staff. The patients were classified according to the modalities of treatment as receiving observation, resuscitation, medical care, and minor or major surgical intervention.
Data on patients’ management and treatment outcomes were collected and analyzed. The digital database study records were reviewed and analyzed for factors such as age, sex, sociodemographic data, reason for the injury, type of weapon, site of injury, type of injury, the modality of management, and the outcome. Results were presented as absolute frequencies, percentages, and mean values. IBM SPSS ver. 22 (IBM Corp., Armonk, NY, USA) was used for data analysis.
RESULTS
In total, 252 Saudi Arabian patients involved in intentional injuries were included. In the same period, the overall total number of emergency cases seen and treated in the emergency department of our hospital was 418,076 patients. Among them, 19,364 patients were diagnosed and treated for all forms of trauma. The proportion of trauma cases among emergency patients at our hospital in 2013 was 4.6%. The proportion of intentional injuries among emergency patients in our hospital in 2013 was 0.1%, and the proportion of intentional injuries among trauma patients at our hospital in 2013 was 1.3% (Fig. 1).
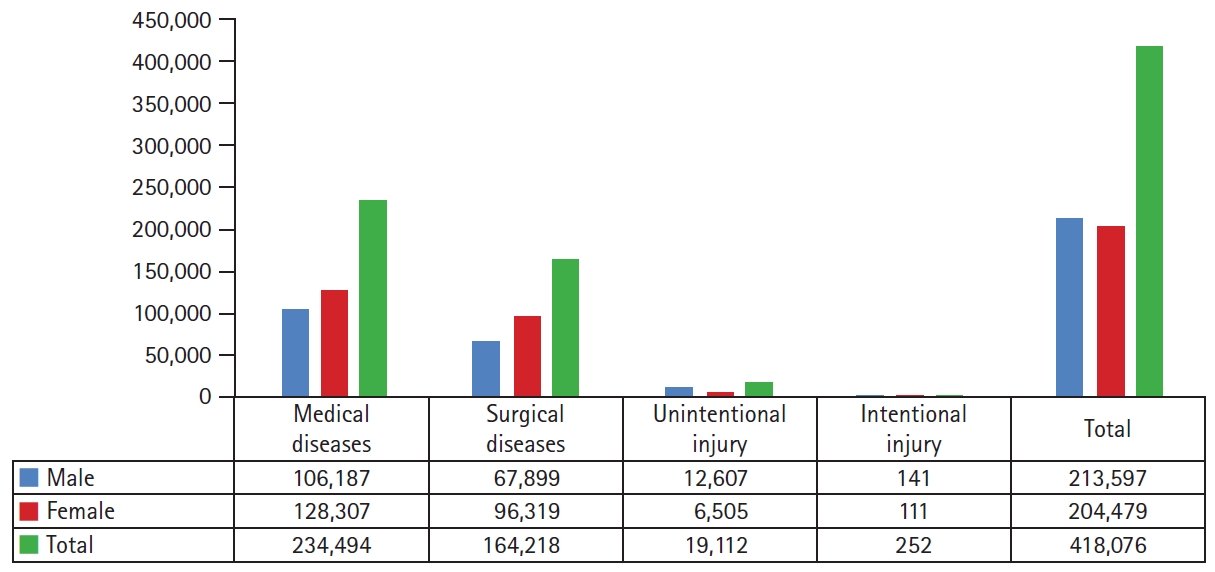
The overall total number of emergency cases seen at Al Ansar General Hospital, Medina, Saudi Arabia during 2013.
The mean age was 34.2±9.4 years (range, 13–57 years). The most common age group was 30 to 40 years (57.9%), followed by 20 to 29 years (32.5%), and 41 to 50 years (4.4%), respectively. An analysis of the distribution of patients by sex showed that 141 patients (56.0%) were male and 111 (44.1%) were female (male to female ratio, 1.27:1). The majority of patients (81.0%) had a formal education, while 16% had a nonformal education and 3% were illiterate. Most patients (n=140, 55.6%) were married, 104 (41.2%) were single, and only eight (3.2%) were divorced. In women, married status showed a significant relationship with intentional injuries (P<0.05).
Although our hospital is a regional trauma primary center, the majority of intentional injury patients were from the city of Medina (n=222, 88.1%), followed by towns and villages (n=23, 9.1%), and rural areas (n=7, 2.8%). The majority of intentional injuries (n=159, 63.1%), occurred at night. Married status showed a statistically significant relationship with night-time intentional injuries (P<0.05). Most of the intentional injuries (n=180, 71.0%), occurred outside the home. Married status showed a statistically significant relationship with outside intentional injuries (P<0.05) (Table 1).

Sociodemographic data of intentional injuries in Saudi Arabian patients
Men were more likely to have night-time injuries (83.0%) and injuries occurring outside the home setting (85.0%) than women, which represented a statistically significant difference (P<0.05) (Fig. 2).
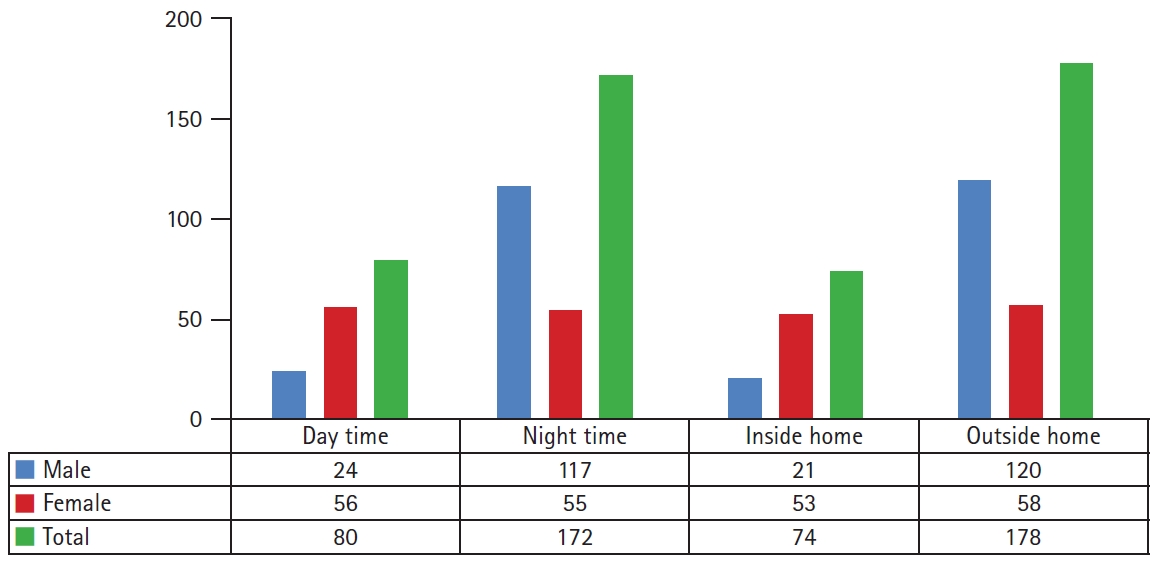
Comparison of the time and setting of intentional injuries in Saudi Arabian patients by sex.
Regarding the reasons for intentional injury, financial problems (n=62, 24.6%) and social disputes (n=61, 24.2%) were the most common. All reasons showed statistically significant relationships (P<0.05) with the male sex, except for sexuality, which had a statistically significant relationship (P<0.05) with the female sex (Table 2).

The distribution of reasons of injury according to sex among Saudi Arabian patients with intentional injuries
Concerning the weapons used in intentional injuries, sharp objects (n=93, 36.9%) were the most common. All weapons showed statistically significant relationships (P<0.05) with the male sex, except for body parts (mainly punching by a fist), which was significantly associated (P<0.05) with the female sex (Table 3).

The relationship between the weapons used and the sex of Saudi Arabian patients with intentional injuries
An analysis of the body parts injured showed that the head and neck were the most commonly injured (n=63, 54.4%), followed by the abdomen (n=41, 12.3%). Injuries to the upper limbs showed a statistically significant relationship (P<0.05) with the male sex, while injuries of the genitalia showed a statistically significant relationship (P<0.05) with the female sex (Table 4).

The relationship between the body parts injured and the sex of Saudi Arabian patients with intentional injuries
Superficial cuts (n=87, 34.5%), were the most common type of injury, and they were found to have a statistically significant relationship (P<0.05) with the male sex. Blunt injuries showed a statistically significant relationship (P<0.05) with the female sex (Table 5).

The relationship between the type of injury and the sex of Saudi Arabian patients with intentional injuries
Suturing of wounds (n=54, 21.4%) and surgical debridement (n=47, 18.7%) were the most commonly performed modalities of management in both male and female patients. Major surgical interventions, cardiopulmonary resuscitation, and fracture treatment showed a statistically significant relationship (P<0.05) with the male sex (Table 6).
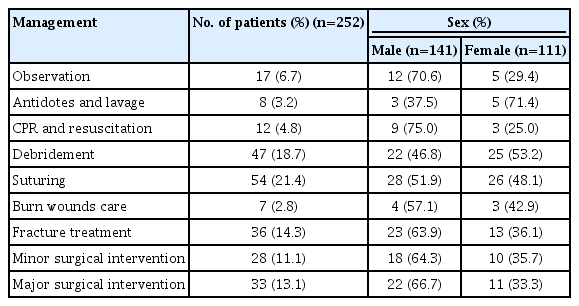
The relationship between the type of management and the sex of Saudi Arabian patients with intentional injuries
A total of 205 patients (81.3%) were treated and discharged, 17 (6.7%) developed a chronic illness, 14 (5.6%) had permanent disabilities, and 14 (5.6%) died (Fig. 3). The majority of patients (n=234, 92.9%), completed their treatment at our hospital, while 18 (7.1%) were resuscitated and transferred to a specialized tertiary hospital for advanced therapies (Fig. 4). An analysis of the mode of transportation showed that 172 patients (68.3%) were brought by ambulance (the Saudi Red Crescent organization), 33 (13.1%) by their parents, 27 (10.7%) by relatives, 11 (4.4%) by neighbors, and nine (3.6%) by themselves (Fig. 5).
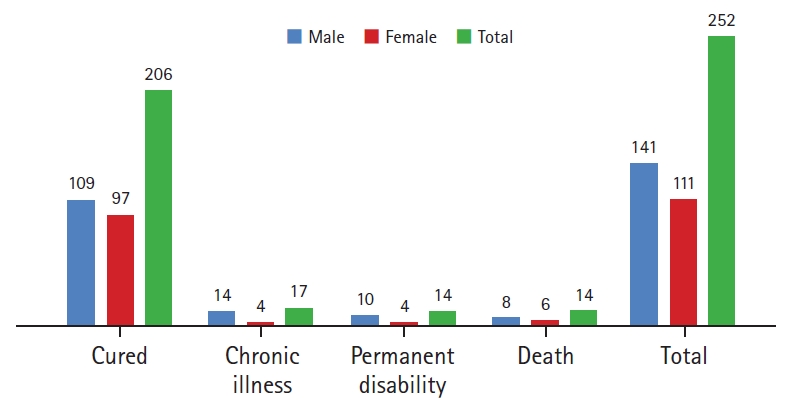
The outcomes of treatment of intentional injuries in Saudi Arabian patients.
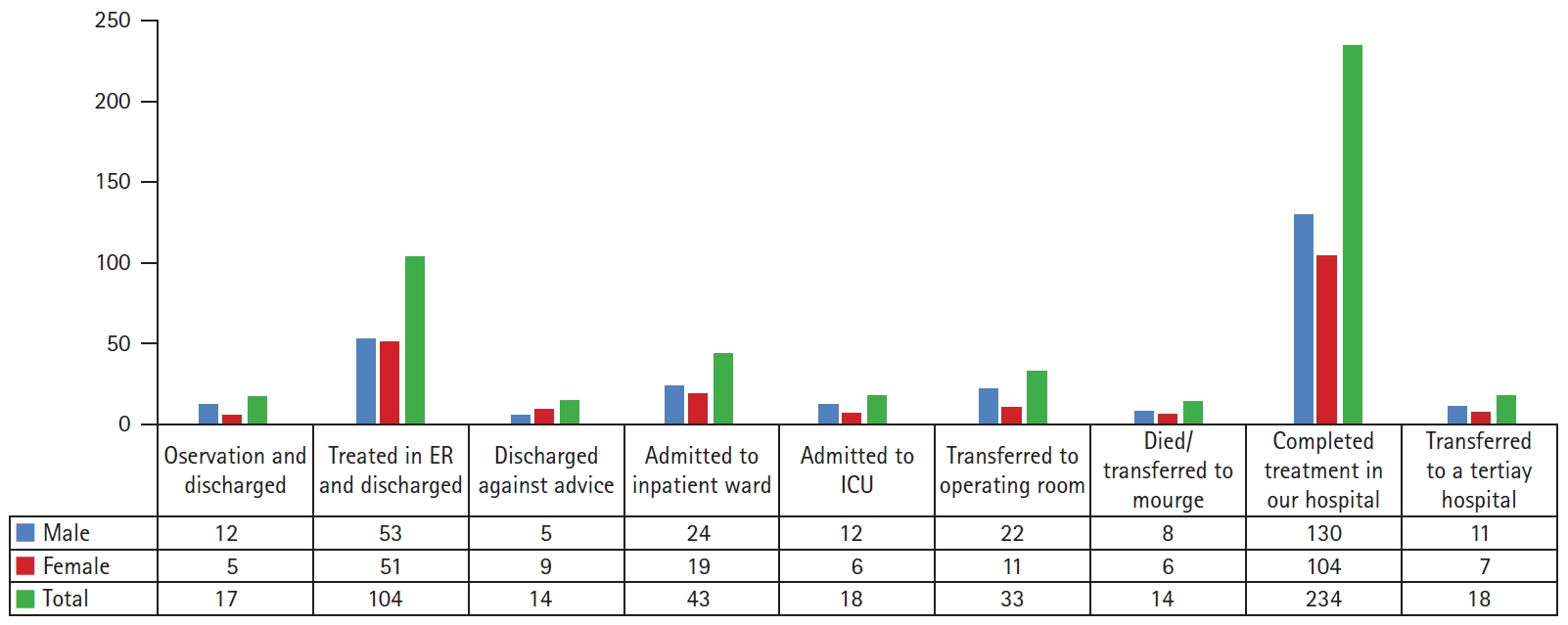
The outcomes of the management of Saudi Arabian patients with intentional injuries. ER, emergency room; ICU, intensive care unit.
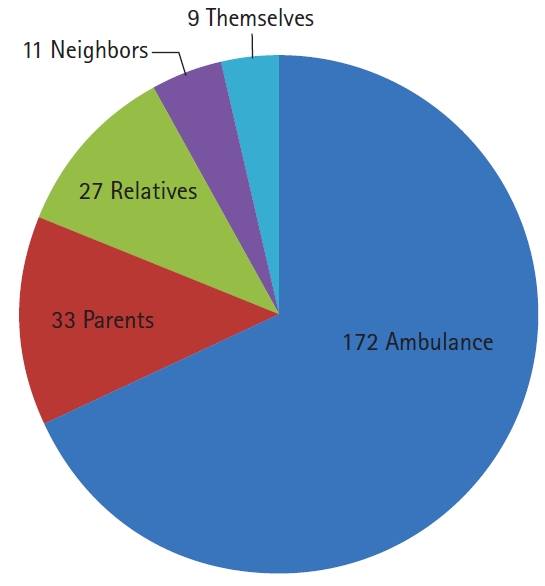
The mode of transportation of Saudi Arabian patients with intentional injuries.
DISCUSSION
From 2012 to 2014, Al Ansar General Hospital, a primary trauma center in Medina, Saudi Arabia, was ranked the top emergency medical center nationwide. In 2013, it received a total of 418,076 patients as emergency cases. As a consequence, a large amount of data was analyzed by several research groups, and we were assigned to investigate trauma patients. This assignment resulted in 11 audit reports, of which this paper is the first product of 18 drafted clinical studies. The amount of clinical data regarding intentional injuries that were retrieved was too vast to be included in a single study, so we had to split it into three separate papers with different kinds of analyzed data.
In our study, the most common age group involved in intentional injuries was 30 to 40 years, which accounted for 57.9% of all patients. Male patients were 1.27 times more common than female, which is similar to the ratios reported by many international published reports [15]. An analysis of the setting of intentional injuries showed that 71% of the cases happened outside the home environment, with male patients being more affected (about 67.4%) than female patients (about 32.6%). This discrepancy could be explained by the social and religious characteristics of Saudi Arabian society, in which men are disproportionately represented in activities outside the house, while women tend to remain at home.
An analysis of the timing of intentional injuries showed that the majority of intentional injuries (n=159, 63.1%), occurred at night. In combination with the finding that 71% of intentional injuries occurred outside the home environment, this finding logically represents aspects of the lifestyle in Saudi Arabia, in which the severely hot daytime weather leads to most social activities (indoor or outdoor) being conducted at night, outside of official working and school hours. Surprisingly, some studies from parts of the world with a cool or moderate climate also reported similar patterns in terms of the majority of injuries occurring outside the home and at night [16].
We observed that the male sex was a risk factor for intentional injuries regarding the timing, setting, reasons for the injury (except sexuality), body parts injured (except genitalia), and the weapons used (except body parts). This finding is logical, since Saudi Arabian society is male-dominant, but it is worth mentioning that the conservative character of Saudi Arabian society could influence the results because women usually fear social scandal and possible punishment or retaliation from their parents (if single) or husbands (if married).
Several international studies reported that a significant number of patients treated for intentional injuries had a history of previous intentional injury or attempts. For instance, Goins et al. [17] reported that in 72 patients, 49% had a previous episode of intentional injury. Poole et al. [18] reported that 61% of 64 patients had a previous episode. Sims et al. [19] reported that 44% of 263 patients sustained another episode of intentional injury within 5 subsequent years. In our study, 49 patients (19.4%) with intentional injuries reported a history of a previous occurrence or attempt of intentional injury, which supports the possibility that the victims of intentional injury are at high risk for future injury.
In contrast to most previously published studies [1–19], financial problems (n=62, 24.6%) and social disputes (n=61, 24.2%) were the most common reasons for intentional injuries in this Saudi Arabian study. The psychological factors underlying these two reasons played a crucial role in the different manifestations of the recorded intentional injuries.
Many research articles have documented a religious impact on adult health-related behaviors and injuries, emphasizing the change from biomedical to psychosocial causes of sickness and death. The researchers found that religion (in its social, environmental, and behavioral forms) appeared to have an impact on health status. A literature review revealed more than 300 scientific studies documenting an association between religion and physical health effects, which has been reported in many sociodemographic groups [20]. In our study, religious reasons for intentional injuries accounted for 4.0%, with a male predominance (70.0%). Although Saudi Arabian society is considered to be conservative and religious, psychological factors again appeared as the main influencing factor (e.g., one patient self-amputated his penis because he used to get an erection when seeing women in the holy mosque [Islamic shrine] at prayer times).
It is well-established scientifically that alcohol and drug abuse is a critical health behavior associated with injuries and death, being responsible for about 120,000 deaths per year, which makes it a key predictor of various forms of injuries and illnesses [21]. Despite the religious and conservative characteristics of Saudi Arabian society which completely forbids alcohol and recreational drugs, they were responsible for intentional injuries in 31 patients (12.3%). This threat has recently gained attention as a potential hazard in Saudi Arabia [22].
Self-poisoning and chemical exposure are two growing problems worldwide that are responsible for a significant proportion of intentional injuries and are estimated to account for 23% of all the self-inflicted injuries globally. The poisons used for deliberate self-poisoning include pesticides, medicines, and rodent poisons. Chemical substances are mostly cleaning detergents [23]. Only 13 cases (5.2%) were recorded in our series in association with deliberate poisoning, a much lower value than has been reported internationally.
Firearms contribute to the majority of homicide and suicide deaths worldwide. Several clinical reports identified firearms and other weapons as potential behavioral risk factors for intentional injury in the form of fighting and suicide attempts [24]. In our study, guns were responsible for intentional injuries in 25 patients (9.9%) while sharp objects (knives, swords, and blades) were reported in 93 (36.9%), despite strict regulations and an embargo against weapons sales and acquisitions in Saudi Arabia.
Most of the patients in our study sustained soft tissue injuries and long bone fractures. The nature and type of injuries often help in understanding the kind of weapon used, which is crucial for medicolegal purposes and surgical treatment [25]. The majority of intentional injuries in our study required surgical intervention, mainly in the form of suturing (n=28, 51.9%), debridement (n=22, 46.8%), fracture treatment (n=23, 63.9%), minor surgical procedures (n=18, 64.3%), and major surgical procedures (n=22, 66.7%), demonstrating the cost and financial impact of dealing with intentional injuries.
The outcomes of the treatment of intentional injuries in Saudi Arabian patients showed that the majority (n=206, 81.7%) were cured, while the mortality rate was 5.6%. Of the 14 dead patients, seven were suicidal, four were gunshot victims, two were self-poisoned, and two were self-burn victims. All these data and results were recorded for 1 year only. They do not represent a full picture of intentional injuries in Saudi Arabia but could provide an overview of clinical patterns in the local community. Unfortunately, this paper is the only study to report intentional injuries from a Saudi Arabian health care facility, as evident from a thorough literature search. More detailed, scientifically structured, and nationwide organized clinical studies are highly recommended.
We conclude that intentional injuries in Saudi Arabian society are a health care hazard that is, unfortunately, underreported. The clinical pattern is similar in most aspects to those that have been internationally reported but differs in certain features due to the specific religious and conservative characteristics of Saudi Arabian society. Nationwide clinical studies are strongly recommended.
Notes
Ethical statements
Ethical approval was granted from the the Ethical Committee of Al Ansar General Hospital, Medina, Saudi Arabia and the management guidelines and clinical pathway subcommittee of the quality care program at the same hospital. Informed consent was obtained from all individual participants included in this study.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
None.
Author contributions
Conceptualization: HAS; Data curation: HAS; Formal analysis: HAS, AWA; Methodology: BHS; Project administration: IAZ; Visualization: BHS, IAZ, OAS, WAA, MHA, WNA; Writing–original draft: BHS, HAS; Writing – review&editing: OAS, AWA, WAA, MHA, WNA.
All authors read and approved the final manuscript.