Part 2. Clinical Practice Guideline for Trauma Team Composition and Trauma Cardiopulmonary Resuscitation from the Korean Society of Traumatology
Article information
Based on the revised recommendations, the final recommendations were confirmed after collecting opinions from trauma experts, experts from the Korean Society of Traumatology, and research method experts using the Delphi technique (Table 1).

Scores from the Delphi technique (Likert scale 1-9)
SHOULD A TRAUMA UNIT BE ESTABLISHED IN ORDER TO TREAT TRAUMA PATIENTS?
Recommendation
A. A trauma unit must be established in order to treat severe trauma patients (1C).
B. The trauma unit should be activated to respond within an appropriate time relative to the scale of the medical institution (1C).
Evidence summary
1. Configuration of trauma units
It is internationally understood and established that different medical specialists and personnel must work together to treat polytrauma patients. In many developed countries with trauma units, the completion of a professional trauma program such as Advanced Trauma Life Support, the Japan Advanced Trauma Evaluation and Care, or the European Trauma Course is required to join a trauma unit. Multiple studies have reported that the establishment of specialized trauma units has many advantages [1-4]. However, no study has evaluated the most appropriate configuration of the trauma unit. The membership of a trauma unit depends on the location and institution-specific circumstances [5-11]. Although some studies have reported that only two doctors are needed to effectively treat trauma patients [12,13], other studies have reported the need to have more than two doctors in the trauma unit depending on the severity of the patient. The interpretation, experience, and education of each trauma unit differ according to local circumstances. It is stated in South Korea’s administrative guideline for trauma centers that a trauma unit must be able to respond within 10 minutes and must consist of general surgeons, thoracic surgeons, neurosurgeons, and emergency medicine physicians. However, only 16 trauma centers meet these criteria, and most emergency departments in South Korea do not satisfy these criteria.
2. The role and qualifications of the team leader
The role of the team leader is to assess patients’ data, consider multiple treatment options, and swiftly decide on a treatment plan. Leadership requires the ability to facilitate communication among members and to work out an interdisciplinary agreement. Hoff et al. [14] reported that the implementation of a team leader led to improvements in the treatment process of a trauma patient. Furthermore, Alberts et al. [15] reported that after the implementation of a “trauma unit leader”, the outcomes of trauma patients improved. The team leader must have superb knowledge regarding the treatment of polytrauma patients and experience in interdisciplinary treatment, which consists of being able to assess the patient depending on the situation, treat and monitor, consult with other medical specialties, adjust the medical team, and explain the decision process in the trauma unit to the patient’s legal guardian. It is important that the interdisciplinary method of treatment does not cause a lag in the treatment process, which underscores the importance of establishing a treatment guideline [14,16,17]. According to a nationwide survey of trauma centers conducted by the American College of Surgeons Committee on Trauma (ACSCOT), onefourth of team leaders were trauma surgeons and one-half were general surgeons [17]. Although it was reported that the time to surgery was faster when the team leader was a trauma surgeon, there was no significant difference in survival outcomes [18]. The main role of the team leader is to manage the trauma unit. The management of a team involves recording the team members’ competencies, and researching and making decisions at every step of diagnosis and treatment through discussion and agreement. In trauma, a team leader must possess the ability and qualifications to follow standard guidelines through an interdisciplinary approach to medicine [19].
3. Response time
The response time is defined as the time from the patient’s arrival to the initiation of treatment by the trauma team doctor [20]. The response time allowed for level I and II trauma centers is 15 minutes, whereas for level III and IV trauma centers, the maximum allowed response time is 30 minutes. According to a study conducted by the Trauma Audit and Research Network, the inclusion of a trauma surgeon significantly reduced the mortality rate from 60% to 32% for trauma patients [21]. Luchette et al. [22] reported that when a trauma doctor resides in the hospital, the diagnosis was quicker and the operation was also faster. However, in cases of severe thoracic and head trauma, the time to intensive care treatment was not affected [1,2,10]. Wyatt et al. [23] reported that when an experienced doctor treated severe trauma patients (1,427 patients, injury severity score [ISS] >15), the survival rate was higher than when doctors without much experience treated these patients. It is also recommended that acute trauma patients be reevaluated within 24 hours of their initial treatment in order to prevent additional complications.
Although trauma centers in South Korea are not graded, the 16 trauma centers that exist function as level I centers. Therefore, it was determined that this clinical practical guideline was acceptable and applicable within South Korea.
SHOULD ACTIVATION OF THE TRAUMA UNIT BE STRATIFIED DEPENDING ON THE SEVERITY OF THE TRAUMA INJURY?
Recommendation
A stratified response system maximizes medical resources and thus should be considered (2B).
Evidence summary
1. Activation of the trauma unit
In an effective trauma system, the patient’s status and severity must be determined and the patient must be transported prior to activating the trauma unit. Not only does the matrix triage system provide a more efficient way to treat severe trauma patients, but it also reduces transportation costs. The American Trauma Society states that 25% to 35% patients are overtriaged, whereas 5% are undertriaged [20]. However, when the sensitivity of the goal was set to 80%, a study was not able to reduce the ratio of underestimation to lower than 70% [24]. Accordingly, the ACSCOT responded by publishing a standard matrix triage system, which has proven to be more efficient. A study utilizing the ACSCOT matrix triage system conducted at a level I trauma center with 7,031 trauma patients reported that matrix triage system yielded a 45% rate of overestimation and a 24% rate of underestimation [25]. Since a stratified medical system maximizes medical resources, the application of such implementation of such systems may be considered for South Korea.
WHAT ARE APPROPRIATE PHYSIOLOGICAL CRITERIA FOR TRAUMA UNIT ACTIVATION?
Recommendation
The physiological criteria for trauma unit activation are the following (1B):
A. Respiratory rate <10 or >30 breaths per minute
B. Systolic blood pressure <90 mmHg
C. Heart rate >100 bpm
D. Glasgow coma scale (GCS) <13
The criteria for trauma unit activation according to the 2016 operating instructions for trauma centers in South Korea are as follows:
1. Physiological indications
A. Airway obstruction/Decreased respiratory rate
B. Intubation prior to arrival
C. Adults: Respiratory rate <10 or >30 breaths per minute
D. Adults: Systolic blood pressure <90 mmHg
E. Adults: heart rate >100 bpm
F. GCS <13
G. A transferred patient undergoing blood transfusion to maintain vital signs
H. Worsening status of a stabilized patient
2. Anatomical criteria
A. Penetration injury
i. Penetrating injury to the craniocervical, thoracic, or abdominal region
ii. Limbs: Penetrating injury proximal to the elbow or knee
B. Thorax
i. Chest wall instability or deformity (e.g. flail chest)
C. Nervous system
i. Open or depressed skull fracture
ii. Quadriplegia or suspicion of spine injury
D. Orthopedic
i. Pelvic fracture
ii. Two or more proximal long-bone fractures
iii. Crushed, degloved, mangled, or pulseless extremity
iv. Amputation proximal to wrist or ankle
3. Mechanism of injury
A. Death in the same passenger compartment
B. Ejection (partial or complete) from an automobile
C. Traffic collision at over 60 km/h
D. Automobile versus pedestrian/bicyclist: thrown, run over, or with significant (over 30 km/h) impact
E. Rescue time exceeding 20 minutes
F. Motorcycle, bicycle, etc.: collision over 30 km/h or roll-over accident
G. Fall greater than or equal to: 6 m for adults, 3 m for children
H. Injury from an explosion
※ When deemed necessary by a clinician in the resuscitation area.
Evidence summary
1. Blood pressure and respiratory rate
Low blood pressure in trauma patients is correlated with a 1.6-fold increase in emergency operations, a 24-fold increase in the mortality rate, and a 7-fold increase in the need for intensive care unit (ICU) treatment [26]. The ACSCOT implements low blood pressure as a criteiron for transporting the patient to the trauma center, whereas hospitals in the state of South Wales in Australia use blood pressure as an indicator for activating the trauma unit [20,27]. Furthermore, in a study conducted by New York’s trauma registry, low blood pressure and a respiratory rate of <10/min or >29/min were correlated with mortality rates of 32.9% and 28.8%, respectively [28].
2. GCS
According to Kohn et al. [29], 44.2% patients with a GCS score of less than 10 were confirmed to have severe brain injury. Although a GCS score of less than 14 was shown to be correlated with the presence of a pathological brain injury [30,31], the need to activate the trauma unit was not implicit (GCS ≤14 and ≥11). In another study, a GCS score less than 10 was correlated with a 3.5-fold increase in mortality during surgery [32]. In the ACSCOT guideline, the indications for trauma activation include a car accident that caused the car to be dented by more than 20–30 inches, a pedestrian hit at the speed of 20–30 mph, or a passenger dying from the traffic accident [20]. It is also stated that a rollover car crash increases the risk of severe trauma [33].
3. Mechanism of injury
When the trauma unit was activated based on the mechanism of injury alone, 92% of cases were overestimated, and the sensitivity and PPV were reported to be 50–70% and 16.1%, respectively [34-36]. However, when the mechanism of injury was included in the criteria, the sensitivity and specificity increased to 80% and 90%, respectively [35]. Kohn et al. [29] reported in a prospective study that 9.4% of patients who fell from a height over 6 m needed ICU care or immediate surgery. Furthermore, Yagmur et al. [37] reported that patients who died from falling injuries fell from heights over 9 m.
4. Age
When Kohn et al. [29] analyzed various trauma activation protocols, such as that of the ACSCOT, it was determined that an age cut-off of over 65 years was most appropriate for activating the trauma unit [29]. Demetriades et al. [38] reported that patients over 70 years of age had a 16% higher mortality rate and a 19% higher likelihood of needing surgical and ICU treatment than younger patients. Mackenzie demonstrated that after the age of 55 years, the risk of fatal trauma injuries significantly increased [39]. Lastly, Grossman et al. [40] reported that patients over the age of 65 had a 6.8% higher mortality rate than their younger counterparts. Since, South Korea uses most of the Centers for Disease Control and Prevention field triage guidelines, it was determined that this clinical practical guideline was applicable within South Korea.
WHAT FACTOR S SHOULD BE CON SID - ERED WHEN CARDIOPULMONARY RESUSCITATION (CPR ) IS BEING PERFORMED IN TRAUMA PATIENTS?
Recommendation
A. Cardiac resuscitation must follow the standard cardiac resuscitation guideline (1A).
B. When CPR is being performed, the correction of reversible causes of cardiac arrest should be performed regularly (1B).
Evidence summary
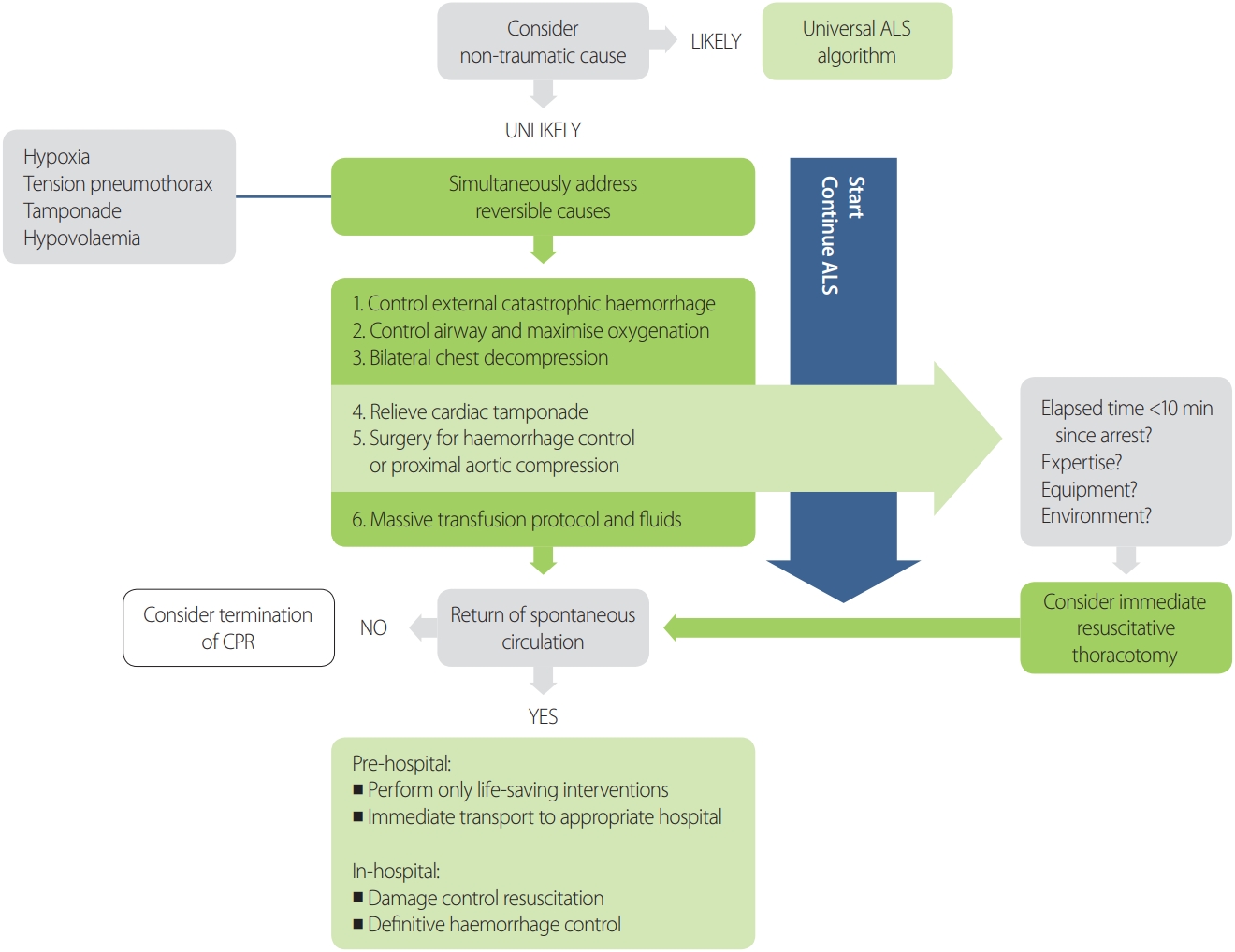
According to the International Liaison Committee on Resuscitation (ILCOR) and the European Resuscitation Council (ERC) guideline, trauma patients receiving cardiac resuscitation should be treated according to standard cardiac resuscitation guidelines [41-44]. The 2015 American and European cardiac resuscitation guidelines recommend that the 5 H’s and 5 T’s (hypovolemia, hypoxia, hydrogen ion [acidosis], hypo/hyperkalemia, hypothermia, tension pneumothorax, cardiac tamponade, coronary thrombosis, pulmonary thrombosis, toxins) or the 4 H’s and 4 T’s must be treated actively during cardiac resuscitation [43,44].
Complications from hemorrhage such as severe brain injury and hypovolemia are the most common cause of cardiac arrest from trauma. Other common causes of traumatic cardiac arrest include other reversible causes such as hypoxia, tension pneumothorax, and tamponade, which must be corrected immediately [43]. Not only does the above guideline recommend assessing, diagnosing, and treating the causes of cardiac arrest of trauma patients as soon as possible, but it states that treating the reversible causes should be prioritized before performing cardiac compressions [43]. In trauma patients, the primary cause of cardiac arrest must be treated by rapidly administering crystalloids and utilizing surgical endoscopic and endovascular techniques to control hemorrhage [44].
Furthermore during the hands-off time of cardiac resuscitation, it is recommended that a trained sonographer perform heart sonography in order to diagnose and treat the cause of hypovolemic cardiac arrest [44]. Some retrospective studies have reported that inserting a chest tube for preventing or treating tension pneumothorax can increase the survival rate for trauma patients with cardiac arrest [45-48].
In the S3 guideline published by the German Trauma Society (DGU), 10,359 patients in the trauma registry were analyzed. In this study the survival rate of trauma-induced cardiac arrest patients was 7.8% when the patient was treated with thoracotomy at the emergency department. However, the type of trauma was associated with a difference in the survival rate: that of cardiac arrest caused by blunt trauma was 1.6%, whereas that of cardiac arrest caused by penetrating trauma was 11.2% [49-51]. Lastly it is recommended by the EAST guideline that cardiac arrests caused by penetrating trauma injuries should be treated with emergency thoracotomy [52].
The DGU S3 guideline implemented much of the 2005 ERC guideline, and it was determined that a more updated guideline would be needed. In the ERC and AHA 2015 guideline, policies were implemented from the 2010 recommendations without further review. Since the ERC guideline presents a thorough algorithm for performing CPR in cases of trauma, it was determined that the cardiac arrest algorithm from the ERC guideline would be implemented (Fig. 1).
WHAT INDICATORS SHOULD BE USED TO MONITOR TRAUMA PATIENTS WITH CARDIAC ARREST?
Recommendation
A. When a trauma patient is being treated with cardiac resuscitation, end-tidal CO2 is recommended to be used as an indicator to decide whether to terminate resuscitation treatment and to predict the patient’s death (1B).
B. Although arterial cannulation can objectively measure the efficiency of CPR and help diagnose cardiac arrest, cannulation must not delay or stop the process of CPR (2C).
Evidence summary
Physiological indicators can be helpful alongside clinical signs and electrocardiograms when performing CPR. However, no recommendations exist regarding which specific physiological indicator(s) should be used to determine the need for CPR. This fact stems from the concern that the evidence used to determine the need for CPR could actually do more harm than good. End-tidal CO2 (ETCO2) should not be used alone to predict death and the termination of CPR [46], but ETCO2 can be recommended for use as a threshold value [53].
The initiation time of CPR should be determined by the readings of an electrocardiogram and signs of cardiac arrest [54]. Pulse oximetry and capnography readings are essential for polytrauma patients and can be used during cardiac arrest. However, the limitations of such indicators for patients in shock or hypothermia should be noted [44]. To assess the quality of CPR, the intubation tube must be placed in the correct location, and waveform capnography can be used to monitor the return of spontaneous circulation [54].
According to the S3 guideline, early catheterization of the femoral artery can be used to continuously measure blood pressure, help diagnose cardiac arrest in the emergency room, and objectively measure the effectiveness of CPR. However, it was recommended that catheterization must not delay or stop the process of CPR [44].
In the ERC and AHA 2015 guidelines, policies were implemented from the 2010 recommendations without further review. In the DGU S3 guideline on cardiac resuscitation, much of the information was based on the ERC 2005 guideline. Therefore, these guidelines should be updated.
WHAT SITUATIONS REQUIRE CPR TO BE INITIATED AND TERMINATED FOR TRAUMA PATIENTS?
Recommendation
A. Termination of CPR must be considered when resuscitation is not successful after the reversible cause of cardiac arrest is corrected (1C).
B. CPR termination must be considered if the patient is determined to have deceased or exhibits signs and injuries that are unlikely to be survivable (1C).
Evidence summary
In a previous study conducted throughout the 1980s to the 1990s, the ERC reported that cardiac arrest trauma patients had a survival rate below 2%. However, according to a German and American study conducted using cardiac arrest trauma patients from the DGU registry, the survival rate of such patients was 17.2% and 13% respectively, a higher rate than was previously thought [55,56]. It must be noted, though, that the American study only included cardiac arrest patients who arrived within the ICU bay within 1 hour.
If the health care provider is unable to find a pulse, or other clinical signs suggesting cardiac arrest, the health care provider must without hesitation start CPR. The clinical guideline for detecting cardiac arrest is no different in trauma than in other situations. The need for CPR should be determined according to the AHA or ERC guideline [57].
Determining the need for CPR by pulse must take no longer than 10 seconds. If this time is exceeded, CPR is performed whether a pulse was found or not. Simultaneously checking the absence of breathing and gasping, which occurs within 5 minutes in 40% of cardiac arrest patients, and the pulse of the patient is ideal so that the time to perform CPR is not postponed [58,59]. Furthermore, seizures must be recognized as a symptom of cardiac arrest [59].
The cessation of CPR is determined by the possibility of successful resuscitation or an underlying clinical judgment of a failed attempt at resuscitation. Furthermore, the cessation of CPR does not need the approval of the patient or caretaker; thus, if the caretaker demands CPR for a patient in whom it would be meaningless, the health care providers must explain that continuing CPR would be meaningless and cease performing CPR. The continuation of meaningless CPR can worsen the ability to make logical judgments and provide false hope for the patient and his or her caretaker. The decision to cease CPR should be explained as a means to stop causing further damage and to maximize the comfort and quality of life for the patient, instead of as a decision to give up [60].
Most initial deaths of polytrauma patients are caused by severe traumatic brain injury and massive hemorrhage. Furthermore, injuries without a possible survival outcome may occur (e.g., aortic injuries). The success of CPR depends on two factors: first, the time of performing CPR after cessation and second, the removal of a reversible cause of cessation of the heart. The typical reversible causes of traumatic cardiac arrest are shock caused by hemorrhage, tension pneumothorax, and cardiac tamponade. Some other causes such as severe brain damage and aortic injury are near-impossible to treat in the acute phase. Even if the cause of cardiac arrest is removed, CPR may fail, and CPR must be ceased if cardiac arrest continues and the cause of cardiac arrest cannot be found. The clinical sign of death must reflect irreversible death of essential organs at the cellular level and can be used as a marker for predicting the failure of CPR. If the patient dies, there is no possibility of survival, and there are clinical signs of cellular injury, CPR must be ceased. The decision to continue or cease CPR must be decided through the discussion of the medical staff involved in the process of CPR. There is no time indication for the failure of CPR. If the patient is eligible for organ donorship, once CPR is ceased, the patient can be considered for transportation to a medical facility for organ donation [60].
Although the American College of Surgeons and the National Association of EMS recommends the cessation of CPR for cardiac arrest trauma patients with no pulse, respiration, or detectable electrical pulses on an electrocardiogram [61], there have been cases where such patients have made full neurological recoveries. Thus, following these guidelines is recommended [62]:
In the following situations, CPR cessation for traumatic arre st should be considered:
- If after 15 minutes, no signs of life are detected
- For severe traumatic injuries (e.g., severe injuries such decapitation, penetrating cardiac injuries, and the outflow of brain tissue), where the likelihood of survival is low
- After a reversible cause of cardiac arrest is confirmed and corrected, but spontaneous circulation is not established.
- When cardiac activity cannot be seen on cardiac ultrasound.
It was determined that this clinical practical guideline is applicable within South Korea. Since the initiation and cessation of CPR faces many legal problems, making a decision at the prehospital phase is a hard task. However, this guideline considers traumatic cardiac arrest patients for in-hospital situations and was therefore determined to be applicable within South Korea.