Thoraco-laparotomy approach to salvage a life-threatening cardiac box stab injury to the infecrior vena cava in Malaysia: a case report
Article information

Abstract
Torso stab injuries near the cardiac box may present unique challenges due to difficulties in hemorrhage control. For a stab injury to the heart, the repair is straightforwardly performed via median sternotomy. In contrast, injuries to the inferior vena cava are challenging to repair, especially when they are close to the diaphragm, and the bleeding can be torrential. Herein, we describe a case of a self-inflicted stab wound within the "cardiac box." The trajectory of the stab injuries went below the diaphragm and injured the infradiaphragmatic inferior vena cava. Successful emergent repair via the thoraco-laparotomy approach revived the young man. In this report, we revisit and discuss previous large series of patients with this rare vena cava injury.
INTRODUCTION
Torso stab injuries near the “cardiac box” may present unique challenges due to difficulties in hemorrhage control, especially when the trajectory is bi-cavitary. Patients may experience injuries to the cardiac, lung, or great vessels (vena cava, aorta, or subclavian vein), requiring urgent operative repair. A recent large series from a level I center observed 23 stab injuries to the cardiac box in a 6-year period. The largest category (15 of 105) was cardiac injuries, followed by lung injuries, great vessel, or smaller artery injuries (i.e., injuries to the internal mammary, intercostal, or superior thoracic artery) [1]. In injuries to the heart, the repair is relatively straightforward, with access via median sternotomy. In contrast, injuries to the great vessels—in particular, the inferior vena cava (IVC)—are challenging to repair. It is worst when the vena cava tears below and close to the diaphragm, and the bleeding can be torrential. Herein, we describe a case of a self-inflicted stab wound within the cardiac box. The trajectory of the stab injuries went below the diaphragm and injured the infradiaphragmatic IVC. A successful emergent repair via the thoraco-laparotomy approach revived the young man from the cardiac box stab injury. The clinical course and operative approach are described in this report; we also compared the current case with previous series describing this rare injury in terms of the approach and reported outcomes.
CASE REPORT
A 35-year-old man was brought to the emergency department with multiple stab wounds within the "cardiac box" 1 hour before arrival. It was assumed to be a suicide attempt based on closed-circuit television recordings. He was hypotensive and received early blood transfusions to sustain a systolic pressure of 90 mmHg. He was very tachycardic, with a heart rate of 143 beats/min, and his Glasgow Coma Scale score was 3 for the eye component, 1 for the verbal component, and 2 for the movement component, which prompted endotracheal intubation for airway protection. There were three stab wounds within the cardiac box, each measuring 2 to 4 cm in length (Fig. 1). A focused assessment with sonography in trauma scan was positive for free fluid in both the right upper quadrant and pericardium (Video S1). His initial hemoglobin level was 13.1 g/dL, and the chest radiograph featured a widened mediastinum shadow (Fig. 2). He was immediately rushed to the operating room (OR). In total, prior to OR entry, he was resuscitated with 1 L of crystalloid, 1 g of tranexamic acid, and 2 units of safe O with a concurrent massive transfusion protocol (MTP). We carried out hypotensive resuscitation, and MTP was continued in the OR. A thoraco-laparotomy (via a sternotomy and midline laparotomy) found three stabs wound trajectories. The first wound trajectory resulted in a large diaphragm laceration, extending to the liver and further into the pericardium. It pierced the IVC, which was bleeding profusely. The IVC perforation measured 0.5×1 cm, and it was repaired following the division of the diaphragm for adequate exposure (Fig. 3). There were also pericardial lacerations from the other two tracts measuring 2 and 3 cm, respectively; these severed the left internal mammary artery, which could be easily controlled.

Multiple stab wounds over the cardiac box.

Chest radiograph showing a widened mediastinum.
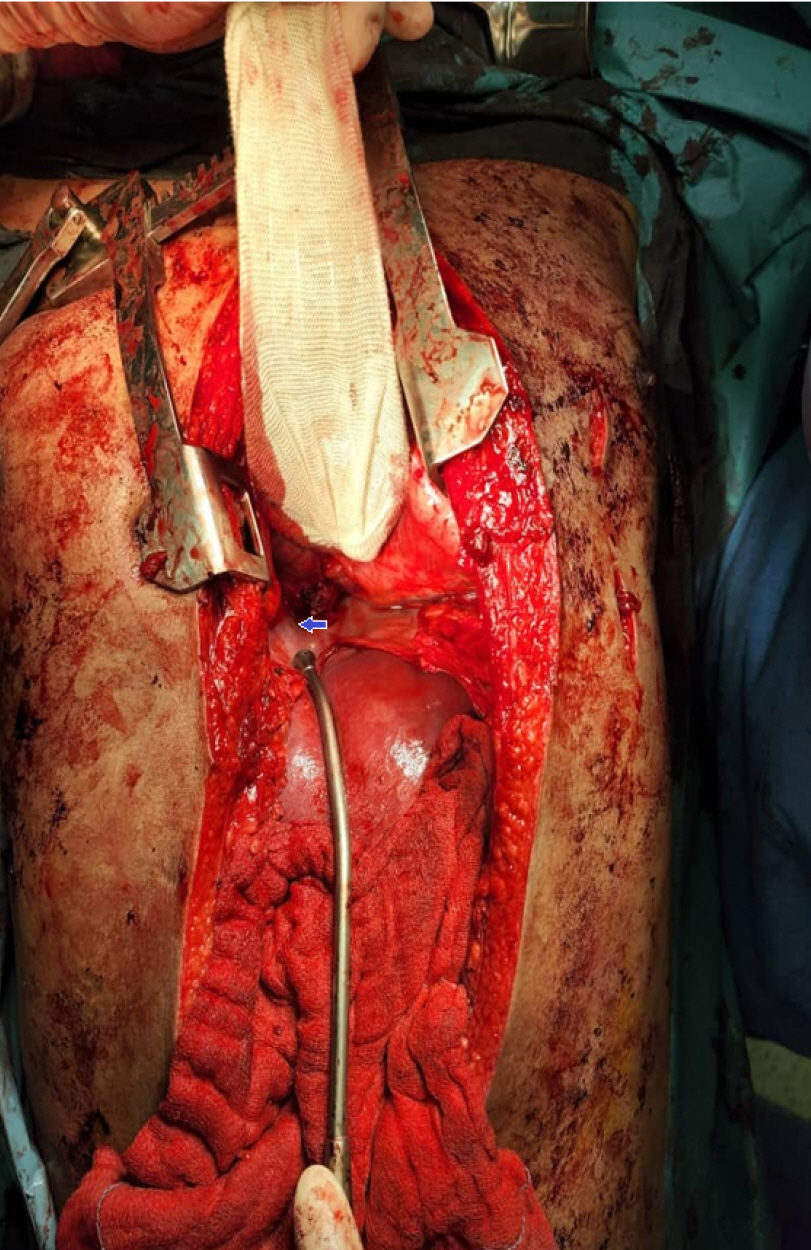
Exposure of the inferior vena cava following its repair.
Massive blood loss occurred during the survey, necessitating activation of the MTP for trauma. In total, 6 units of packed cells, 8 units of fresh frozen plasma, 6 units of cryoprecipitate, and 4 units of platelets were transfused intraoperatively. To make matters worse, the patient was also positive for COVID-19; thus, the operating team had to operate wearing full personal protective equipment. The patient had to be treated in a full-isolation intensive care unit postoperatively and was extubated on day 8 following surgery. After another week in the hospital, he recovered well; however, he absconded before being discharged and did not return for follow-up.
Ethics statement
Written informed consent was obtained from the patient for the publication of this case report and accompanying images. The authors conformed to the provisions of the Declaration of Helsinki.
DISCUSSION
Injuries to the IVC carry a high mortality rate, up to 53%, according to the older series [1]. Mortality increases with the proximity of the wound to the heart [2]. The majority of the literature contains American data, with injuries mostly arising from the infradiaphragmatic segment of the IVC and repaired through abdominal access [2]. The mechanism of injury was due to penetrating trauma three-fourths of the time, but the survival outcomes did not vary according to the mechanism [2]. Firearms were reported as the most common mode of injury in another American series, followed by stab wounds and blunt trauma [3]. The operative strategies described included direct compression and local clamping, followed by primary repair of the vein defect. In a few extreme cases, cava ligation was performed [3]. In the follow-up from the previous series, merely primary repair was sufficient, with low rates of thrombosis and embolic complications [3].
An American level I trauma center observed 105 stab wounds in the cardiac box over a period of 6 years. Thirty percent required an exploration via thoracotomy, sternotomy, or laparotomy. Twenty-three patients needed thoracotomy or sternotomy, and 12 patients needed laparotomy. Great vessel injuries were seen in only two cases. The detailed approach was not described [4]. However, another recent case, also from a trauma center in the United States, described a successful repair of an injury to the supradiaphragmatic IVC caused by blunt trauma. The authors concluded that the factors for success included aggressive prehospital fluid resuscitation, facile transfer to the OR, early detection of the injury, an early call for cardiothoracic surgery, and prompt blood transfusion. The details of the operative steps included median sternotomy, placement of a hemostatic patch over the confluence of the IVC and the right atrium and holding it in place, exploration of the abdomen (finding small lacerations of the liver), and supraceliac aortic clamping together with maintaining digital pressure over the IVC in the pericardium. When cardiothoracic surgeons were called in for cardiopulmonary bypass (CPB), the diaphragm was taken down to the caval hiatus to expose the entire suprahepatic IVC, and the IVC was repaired with a Dacron graft. Surgery was performed with deep hypothermic circulatory arrest, as there was no area for adequate clamping of the IVC [5]. On the contrary, in this reported case, we did not need to call in a cardiothoracic surgeon for CPB, as the penetrating injury resulted in a linear tear that could be repaired by oversewing. Furthermore, no emergency CPB service was available at the local center. In short, we summarized the success in the current case as being due to a few factors, which may be similar to those described in previous reports of blunt supradiaphragmatic IVC injuries. These factors include the following: (1) hemostatic resuscitation with an MTP; (2) early detection of a severe injury needing operative repair based on a clinical judgment of a stab box injury together with positive fluids seen on sonography; (3) penetrating injuries characterized by a linear tear pattern with a low concomitant traumatic injury burden; and (4) the presence of a senior trauma surgeon, senior anesthesiologist, and emergency trauma team care providers, as the patient arrived in the early hours.
A review by Chinese authors described a series of IVC injuries. In the current case, the IVC injury was classified as a segment 1 injury, lying between the right atrium and the second hepatic hilum [6]. Injuries around this region carry the highest risk of mortality due to its difficult access, as it hides behind the diaphragm or inside the pericardial sac. It has also been observed that injuries closer to the right atrium have a higher risk of mortality [2]. The older literature on IVC injuries from the United States contains larger series of suprahepatic IVC injuries. Operative repair includes primary repair, patch repair, or ligation. The latter two options often carry a high risk of mortality and poorer outcomes. Nearly 70% of IVC injuries reported in the older large series were due to gunshot wounds, while only 17% were due to stab wounds [4].
The current case described a severe self-inflicted stab cardiac box injury. The patient successfully survived after emergency chest and abdomen exploration, together with IVC repair. The previous literature from the United States observed a high risk of mortality with injury at this segment of the IVC. We summarized a few salient management strategies such as hemostatic resuscitation, early exploration, and an operative strategy involving a large thoraco-laparotomy incision allowing quick local clamping and vein repair to achieve hemorrhage control of bleeding in segment 1 of the IVC.
SUPPLEMENTARY MATERIALS
Video S1.
The presence of free fluid within the pericardial sac.
Supplementary materials are available at: https://doi.org/10.20408/jti.2022.0071.
Notes
Author contributions
Conceptualization: IAM, JHT; Data curation: JZT, YM; Writing–original draft: IAM, JHT; Writing–review & editing: JHT, YM, IAR. All authors read and approved the final manuscript.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
The authors did not receive any financial support for this study.
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.