Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(2); 2023 > Article
-
Original Article
Thoracolumbar spine fracture patterns, etiologies, and treatment modalities in Jordan -
Ahmad Almigdad, MD
 , Sattam Alazaydeh, MD, Mohammad Bani Mustafa, MD, Mu'men Alshawish, MD, Anas Al Abdallat, MD
, Sattam Alazaydeh, MD, Mohammad Bani Mustafa, MD, Mu'men Alshawish, MD, Anas Al Abdallat, MD -
Journal of Trauma and Injury 2023;36(2):98-104.
DOI: https://doi.org/10.20408/jti.2022.0068
Published online: April 14, 2023
- 1,869 Views
- 103 Download
Department of Orthopedic Surgery, Royal Rehabilitation Center, King Hussein Medical City, Royal Medical Services, Amman, Jordan
- Correspondence to Ahmad Almigdad, MD Department of Orthopedic Surgery, Royal Rehabilitation Center, King Hussein Medical City, Royal Medical Services, Amman 11855, Jordan Tel: +962-77-987-8345 Email: akmigdad_just@yahoo.com
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- Spine fractures are a significant cause of long-term disability and socioeconomic burden. The incidence of spine fractures tends to increase with age, decreased bone density, and fall risk. In this study, we evaluated thoracolumbar fractures at a tertiary hospital in Jordan regarding their frequency, etiology, patterns, and treatment modalities.
-
Methods
- The clinical and radiological records of 469 patients with thoracolumbar fracturesadmitted to King Hussein Medical City from July 2018 to August 2022 were evaluated regarding patients’ age, sex, mechanism of injury, fracture level and pattern, and treatment modalities.
-
Results
- The mean age of patients was 51.24±20.22 years, and men represented 52.7%. Compression injuries accounted for 97.2% of thoracolumbar fractures, and the thoracolumbar junction was the most common fracture location. Falling from the ground level was the most common mechanism and accounted for half of the injuries. Associated neurological injuries were identified in 3.8% of patients and were more common in younger patients. Pathological fractures were found in 12.4% and were more prevalent among elderly patients and women.
-
Conclusions
- Traffic accidents and falling from height were the most common causes of spine fractures in patients younger than 40. However, 70% of spine fractures in women were caused by simple falls, reflecting the high prevalence of osteoporosis among women and the elderly. Therefore, traffic and work safety measures, as well as home safety measures and osteoporosis treatment for the elderly, should be recommended to reduce the risk of spine fractures.
- Spine fractures are a significant cause of long-term disability and socioeconomic burden [1,2]. The incidence of spine fractures tends to increase with age, decreased bone density, and fall risk. However, increasing road traffic accidents have led to a higher frequency of spine injuries in young people [3,4].
- Spinal injuries can result from injury to bony structures and the surrounding ligaments [5]. The involvement of the spinal cord may lead to devastating injuries [6]. Thoracolumbar fracture classification systems are used to facilitate effective communication between spine surgeons, guide treatment, and help predict the prognosis. An ideal classification system should be simple, comprehensive, reliable, and reproducible with predictive outcomes. Most of the existing classifications have certain advantages and disadvantages. Denis three-column spine model, proposed in 1989, was subsequently used to develop the AO classification of spinal injuries, which includes three categories: compression fracture (group A), distraction injury (group B), and translational injury or rotational injury (group C), and the severity and the need for surgery increase from group A to C [7–9].
- Thoracolumbar junction fractures (T10 to L2) are the most common spinal column injuries because of the large amount of biomechanical stress involving this region due to the transition from the less mobile thoracic spine to the dynamic lumbar spine [10]. In this review, we evaluated the frequency, etiology, patterns, and treatment of thoracolumbar fractures at a tertiary hospital in Jordan.
INTRODUCTION
- Ethics statements
- This study was approved by the Human Research Ethics Committee of Royal Medical Services (No. 23/2022). The requirement for informed consent was waived due to the retrospective nature of the study.
- Study design
- This retrospective study reviewed the clinical and radiological records of all thoracolumbar fractures admitted to King Hussein Medical City (Amman, Jordan), from July 2018 to August 2022. King Hussein Medical City is a referral center for all districts and health sectors in the kingdom. In total, 469 thoracolumbar patients with fractures were enrolled in this study, their sociodemographic data were extracted from their records, and their radiographs were reviewed using a picture archiving and communication system to analyze the fractures’ locations and patterns.
- The patients’ age, sex, mechanism of injury, level of fracture, fracture pattern, and treatment modalities were obtained. The AO classification system was used to classify fractures into type A (compression injuries, including wedge, burst, spinous, and transverse process fractures), type B (distraction injuries, as represented by Chance fractures), and type C (torsional injuries, which result in fracture-dislocation).
- Treatment was classified as conservative, kyphoplasty, vertebroplasty, and fusion. The mechanism of injury was classified into simple falls (from ground level), falls from height, road traffic accidents, and others. Age groups were classified into 18 to 40, 40 to 64, and older than 65 years. Pediatric patients (younger than 18 years) were excluded from the study.
- Statistical analysis
- The mean and standard deviation were used to describe the continuously measured variables and the median and interquartile range for continuous variables with skewness. The frequency and percentage were used to describe the categorically measured variables. Multiple-response dichotomy analysis was applied to describe multiple-choice variables. The Kolmogorov-Smirnov test was used to assess the statistical normality assumption for metric variables. The bivariate chi-square test of association was used to assess the correlations between categorical variables. However, the continuity-corrected chi-square and the likelihood ratio chi-square test of association were used when the statistical count assumption was violated in some contingency tables with fewer than expected counts for the 2×2 and 2-way tables. IBM SPSS ver. 21 (IBM Corp) was used for the statistical data analysis. The alpha significance level was set at 0.050.
METHODS
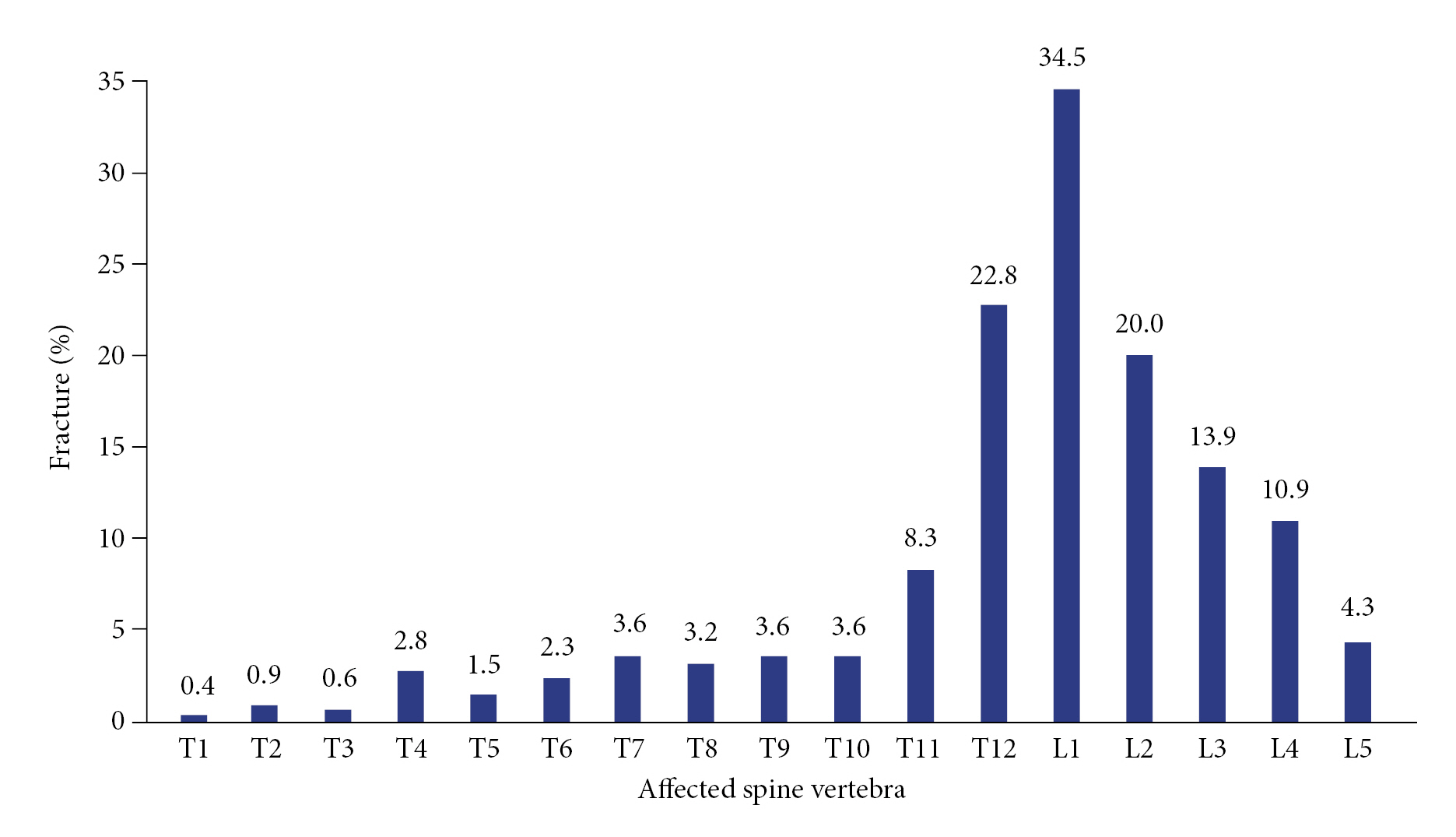
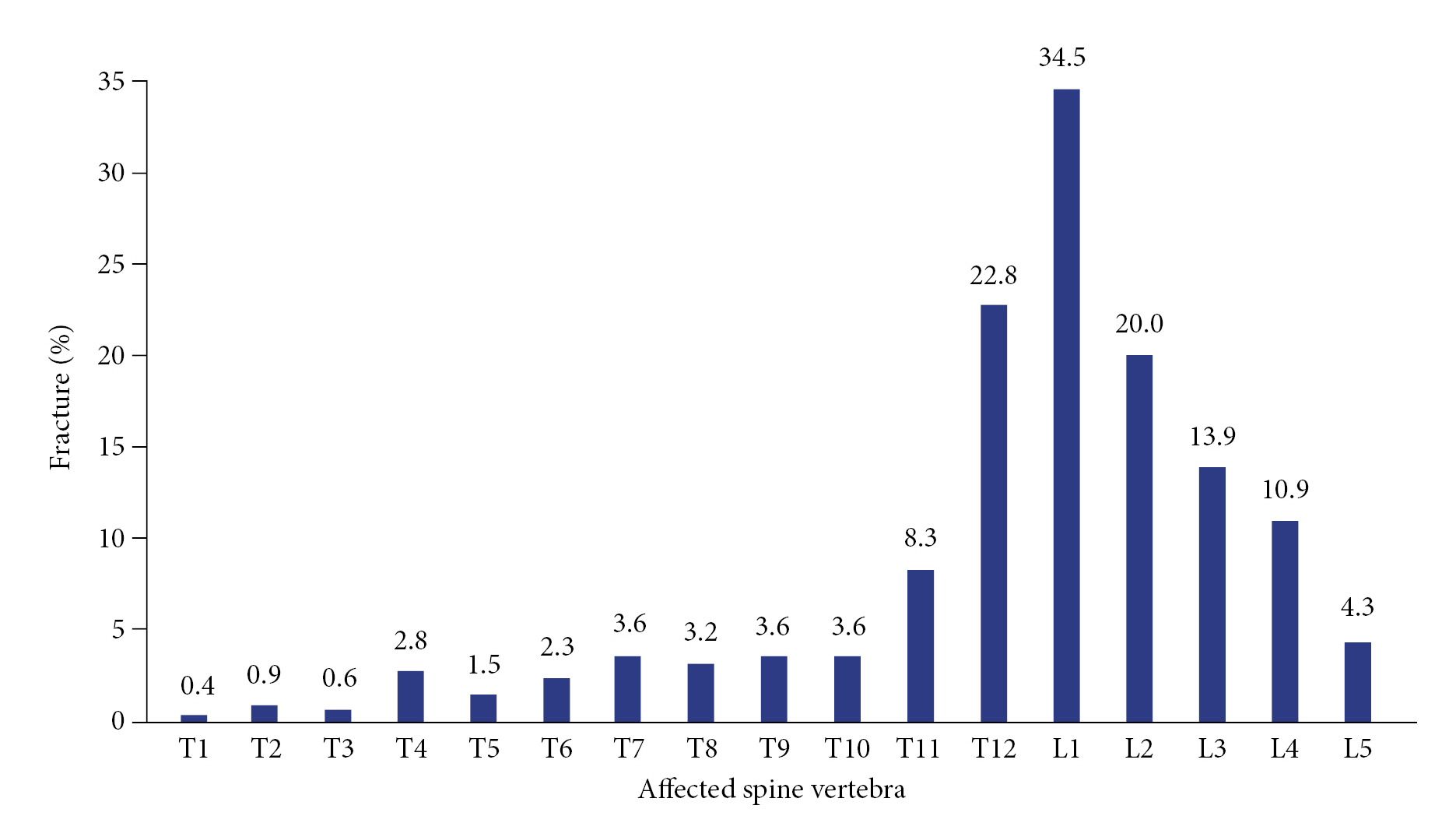
- The records of 469 patients were retrospectively reviewed. The mean age of the patients was 51.24±20.22 years, and male patients represented 52.7% of the sample (Table 1). Compression fractures accounted for most thoracolumbar injuries (97.2%), and wedge and burst fractures were the most common form of compression fractures, accounting for 52.2% and 41.4%, respectively. Distraction and translational injuries represented 2.8% of all injuries. However, associated neurological lesions were identified in 3.8% of patients, and pathologies were found in 12.4%. Injuries mainly occurred in the lumbar spine (83.6%). However, 90% of fractures occurred in the thoracolumbar junction (Fig. 1).
- Falls from the ground level were the most common mechanism, accounting for half of the injuries, while falling from height and road traffic accidents caused 26.7% and 21.3% of fractures, respectively. Most patients (58.0%) were treated surgically, mainly by surgical fusion and kyphoplasty. However, conservative treatment was the treatment for 42.0% of patients.
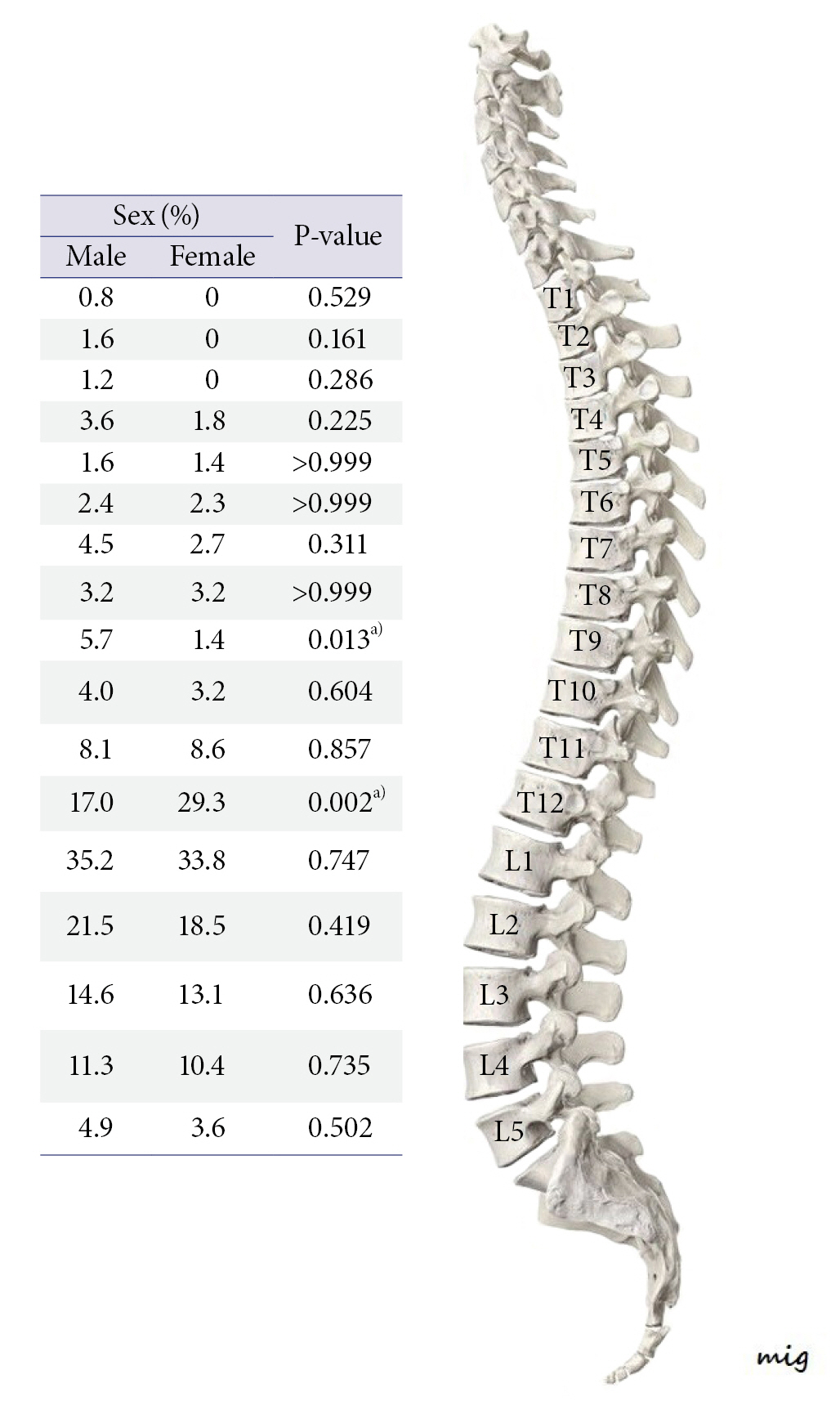
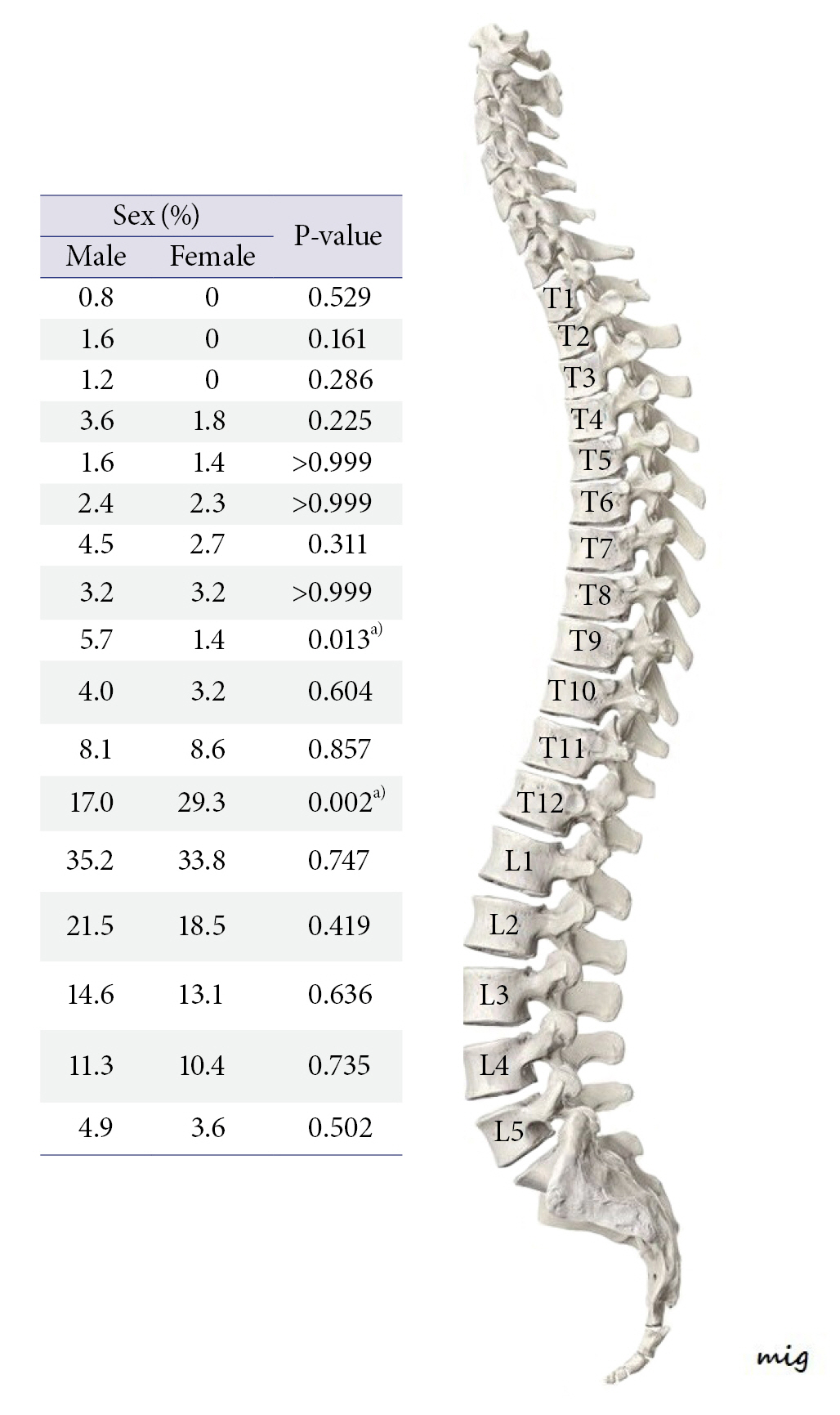
- When comparing the incidence of thoracolumbar fractures between different sexes and ages, more than 50% of thoracolumbar spine fractures in female patients occurred in patients older than 65 years. In contrast, about half of fractures in male patients were observed in patients under the age of 40 years. Additionally, injuries involving higher thoracic spine levels (especially T6 to T9) were significantly associated with younger age groups. Nevertheless, there was no significant difference in lumbar fractures in the different age groups (Figs. 2, 3).
- Compression injuries were the most common pattern across all age groups. Additionally, pathological fractures were more prevalent among the elderly and female patients, and associated neurological injuries were more likely in younger patients. Young patients were more likely to have experienced high-energy injury mechanisms such as falls from heights and road traffic accidents. However, spinal fractures in elderly patients were due to simple falls. Most spine fractures in the younger age group mandated fusion surgery, unlike elderly patients, whose fractures were mostly treated by kyphoplasty (Table 2).
RESULTS
- Epidemiological studies on spinal fractures are lacking in Jordan; thus, this study analyzed thoracolumbar fracture patients admitted to the spine unit in King Hussein Medical City. The results of this study improve our understanding of the incidence of spinal fractures in Jordan, helping to identify the needs of our healthcare system and suggesting guidelines for protective measures.
- The first 10 thoracic vertebrae are connected by ribs to the sternum anteriorly; therefore, the thoracic spine is less mobile than the lumbar spine due to the stability provided by the thoracic cage. In contrast, the thoracolumbar region (T10 to L2) and lumbar region are flexible, and the transition from a less mobile thoracic cage to the lumbar spine explains the high frequency of traumatic spinal injuries and degenerative changes in this region. The spinal cord ends at L1 to L2. Therefore, fractures associated with neurological injuries above this level result in upper motor neuron manifestations and lower motor neuron presentations at a lower level [11–13].
- Many factors play an important role in fracture patterns, such as the mechanism of injury, the age of patients, and preexisting bone pathology. Spine fractures occur mainly with high-energy injuries such as falls and road traffic accidents. Pathological fractures and osteoporotic fractures might happen with minor trauma [14,15].
- When comparing our results with similar studies from other countries in the region—specifically, Saudi Arabia [16] and the United Arab Emirates (UAE) [17]—we found a higher mean age of the patients (51.24±20.22 years) than was reported in the Saudi study (36.9±16.2 years) or the UAE study (37.5±12.5 years). Similarly, in our study, male and female patients were affected nearly equally. However, male patients outnumbered female patients by four times in the Saudi study and nine times in the UAE study. We explain this difference in age and sex as resulting from the large number of expatriate workers in the Gulf area, most of whom are young men. Falling from height was the leading cause of spine injuries in Jordan, while traffic accidents were the most common cause in the Saudi Arabia and UAE studies.
- Simple falls were the most common mechanism of spine fracture in patients older than 40 years. However, it was responsible for 47.2% of injuries in the middle age group and 88.3% for those older than 65 years. In contrast, road traffic accidents were the most common mechanism in young patients, followed by falls from height, and male patients are more prone to such mechanisms.
- Compression injuries are the most common pattern across all age groups and in both sexes. However, the low frequency of minor fractures, such as transverse and spinous process fractures, is explained by the fact that our center is a referral center to which patients whose fractures need surgical intervention or even bracing are referred. In contrast, fractures that did not need such treatment received treatment at the local hospitals distributed throughout Jordan.
- Thoracolumbar fractures were associated with neurological injuries in 3.8% of patients in our study, with no significant difference between the sexes. However, patients younger than 40 were more predisposed to neurological injuries, which is explained by the fact that injuries in this age group are more likely to be due to high-energy injuries such as road traffic accidents and falls from height. Otom et al. [18] retrospectively reviewed 151 patients in Jordan with traumatic spinal cord injuries during 1988–1993 and concluded that the estimated annual incidence was 18 per million population; male patients represented the majority with a percentage of 85.4%, and the mean age was 33 years. Two-thirds of patients developed paraplegia, and the remaining third developed quadriplegia. Motor vehicle accidents were the commonest cause of traumatic spinal injury, followed by bullet injuries.
- Pathological spine fractures accounted for 12.4% of our cases and were more notable in female patients and patients older than 65. However, this percentage would be higher if insufficiency fractures were included. In this study, we defined a fracture as pathological if there were pathological deposits to the spine or radiological reports of pathological fracture. However, some reports counted insufficiency fractures as pathological, although most of these fractures are not classified in the radiological reports as pathological. Therefore, this percentage does not represent the actual prevalence of all pathological fractures, and the lack of sufficient data precludes a detailed analysis of pathological spine fractures.
- The prevalence of osteoporotic vertebral fractures steadily increases with advancing age. Although most fractures heal well, up to 30% of fractures can develop painful nonunion, progressive kyphosis, and neurological deficits. However, such patients will benefit from percutaneous interventions such as vertebroplasty and kyphoplasty, while unstable fractures and associated neurological deficits are candidates for spinal fusion [19,20].
- Thoracolumbar spine fractures can be treated either nonoperatively or operatively, depending on the extent of bony injury, neurological involvement, and posterior ligamentous complex integrity. Most thoracolumbar fractures are stable and treated nonoperatively with a molded brace or hyperextension cast that allows early mobility [21,22]. In our sample, 42% received conservative treatment by bed rest and orthosis; one-third underwent surgical fixation, and 25% received vertebroplasty or kyphoplasty treatment. Young male patients received fusion surgery more often because their high-energy injuries resulted in unstable spine fractures, while female patients more frequently underwent kyphoplasty, which is explained by their higher osteoporotic risk.
- Vertebroplasty or kyphoplasty are minimally invasive vertebral cement augmentation techniques that give an alternative solution to prolonged bed rest or invasive spine surgery. Pain relief occurs due to fracture stabilization and thermal and chemical ablation of nerve endings [23,24].
- The advantage of surgical treatment is that it fastens rehabilitation and early mobilization and allows restoration of surgical alignment of the spine. Surgical intervention allows spinal canal decompression and thus can restore neurological function [25–27]. Surgery carries the risk of blood loss and infection. Rechtine et al. [28] reported a 10% infection rate. Siebenga et al. [29] compared the outcome between a group treated nonoperatively with 5 days of bed rest followed by 3 months of a Jewett brace and another group treated surgically with short-segment posterior pedicle screw fixation and found higher scores in the surgically treated group after 4 years of follow-up.
- The main drawback of our study is the retrospective design, and the lack of adequate documentation of the injury mechanism prevented a detailed analysis of the etiology. Grouping the mechanism of injury into broad categories, such as simple falls and falls from a height, makes it challenging to identify the exact causes of the injury and determine future preventive measures. The lack of data regarding spine pathology precludes a detailed analysis of this issue.
- In conclusion, traffic accidents and falling from heights were the commonest causes of spine fractures in patients younger than 40 years. However, 70% of spine fractures in female patients were caused by simple falls, reflecting the high prevalence of osteoporosis among female and elderly patients. Therefore, traffic and work safety measures should be enforced to reduce the risk of spine fractures in young patients, and home safety measures and osteoporosis treatment should be provided for elderly patients.
DISCUSSION
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Data sharing statement
The data of this article are available from the corresponding author upon reasonable request.
-
Author contributions
Conceptualization: AA; Data curation: SA, MBM, MA, AAA; Formal analysis: AA; Methodology: AA; Project administration: AA; Visualization: all authors; Writing–original draft: AA; Writing–review & editing: AA. All authors read and approved the final manuscript.
ARTICLE INFORMATION
- 1. Mitchell R, Harvey L, Stanford R, Close J. Health outcomes and costs of acute traumatic spinal injury in New South Wales, Australia. Spine J 2018;18:1172–9. ArticlePubMed
- 2. Fechtenbaum J, Cropet C, Kolta S, Horlait S, Orcel P, Roux C. The severity of vertebral fractures and health-related quality of life in osteoporotic postmenopausal women. Osteoporos Int 2005;16:2175–9. ArticlePubMedPDF
- 3. Rajasekaran S, Kanna RM, Schnake KJ, et al. Osteoporotic thoracolumbar fractures: how are they different?: classification and treatment algorithm. J Orthop Trauma 2017;31 Suppl 4:S49–56. ArticlePubMed
- 4. Sidon E, Stein M, Ramalingam G, Shemesh S, Benharroch D, Ohana N. Gender differences in spinal injuries: causes and location of injury. J Womens Health (Larchmt) 2018;27:946–51. ArticlePubMed
- 5. Griffith JF, Guglielmi G. Vertebral fracture. Radiol Clin North Am 2010;48:519–29. ArticlePubMed
- 6. Anandasivam NS, Ondeck NT, Bagi PS, et al. Spinal fractures and/or spinal cord injuries are associated with orthopedic and internal organ injuries in proximity to the spinal injury. N Am Spine Soc J 2021;6:100057. ArticlePubMedPMC
- 7. Vaccaro AR, Schroeder GD, Kepler CK, et al. The surgical algorithm for the AOSpine thoracolumbar spine injury classification system. Eur Spine J 2016;25:1087–94. ArticlePubMedPDF
- 8. Schnake KJ, Schroeder GD, Vaccaro AR, Oner C. AOSpine classification systems (subaxial, thoracolumbar). J Orthop Trauma 2017;31 Suppl 4:S14–23. ArticlePubMed
- 9. Schroeder GD, Harrop JS, Vaccaro AR. Thoracolumbar trauma classification. Neurosurg Clin N Am 2017;28:23–9. ArticlePubMed
- 10. Fradet L, Petit Y, Wagnac E, Aubin CE, Arnoux PJ. Biomechanics of thoracolumbar junction vertebral fractures from various kinematic conditions. Med Biol Eng Comput 2014;52:87–94. ArticlePubMedPDF
- 11. Bogduk N. Functional anatomy of the spine. Handb Clin Neurol 2016;136:675–88. ArticlePubMed
- 12. Adams MA, Dolan P. Spine biomechanics. J Biomech 2005;38:1972–83. ArticlePubMed
- 13. Aulisa L, Pitta L, Padua R, Ceccarelli E, Aulisa A, Leone A. Biomechanics of the spine. Rays 2000;25:11–8. PubMed
- 14. Tang L, Zheng J, Hu J. A numerical investigation of factors affecting lumbar spine injuries in frontal crashes. Accid Anal Prev 2020;136:105400. ArticlePubMed
- 15. Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH. Review paper: epidemiology of traumatic spinal cord injury: comparisons between developed and developing countries. Asia Pac J Public Health 2010;22:9–18. ArticlePubMedPDF
- 16. Alawad MO, Alenezi N, Alrashedan BS, et al. Traumatic spinal injuries in Saudi Arabia: a retrospective single-centre medical record review. BMJ Open 2020;10:e039768. ArticlePubMedPMC
- 17. Grivna M, Eid HO, Abu-Zidan FM. Epidemiology of spinal injuries in the United Arab Emirates. World J Emerg Surg 2015;10:20. ArticlePubMedPMCPDF
- 18. Otom AS, Doughan AM, Kawar JS, Hattar EZ. Traumatic spinal cord injuries in Jordan: an epidemiological study. Spinal Cord 1997;35:253–5. ArticlePubMedPDF
- 19. Capdevila-Reniu A, Navarro-Lopez M, Lopez-Soto A. Osteoporotic vertebral fractures: a diagnostic challenge in the 21st century. Rev Clin Esp (Barc) 2021;221:118–24. ArticlePubMed
- 20. Prost S, Pesenti S, Fuentes S, Tropiano P, Blondel B. Treatment of osteoporotic vertebral fractures. Orthop Traumatol Surg Res 2021;107(1S):102779. ArticlePubMed
- 21. McCarthy J, Davis A. Diagnosis and management of vertebral compression fractures. Am Fam Physician 2016;94:44–50. PubMed
- 22. Goldstein CL, Chutkan NB, Choma TJ, Orr RD. Management of the elderly with vertebral compression fractures. Neurosurgery 2015;77 Suppl 4:S33–45. ArticlePubMed
- 23. Chandra RV, Maingard J, Asadi H, et al. Vertebroplasty and kyphoplasty for osteoporotic vertebral fractures: what are the latest data. AJNR Am J Neuroradiol 2018;39:798–806. ArticlePubMedPMC
- 24. Filippiadis DK, Marcia S, Masala S, Deschamps F, Kelekis A. Percutaneous vertebroplasty and kyphoplasty: current status, new developments and old controversies. Cardiovasc Intervent Radiol 2017;40:1815–23. ArticlePubMedPDF
- 25. Yi L, Jingping B, Gele J, Baoleri X, Taixiang W. Operative versus non-operative treatment for thoracolumbar burst fractures without neurological deficit. Cochrane Database Syst Rev 2006;(4):CD005079. ArticlePubMed
- 26. Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit: a prospective, randomized study. J Bone Joint Surg Am 2003;85:773–81. PubMed
- 27. Chipman JG, Deuser WE, Beilman GJ. Early surgery for thoracolumbar spine injuries decreases complications. J Trauma 2004;56:52–7. ArticlePubMed
- 28. Rechtine GR, Bono PL, Cahill D, Bolesta MJ, Chrin AM. Postoperative wound infection after instrumentation of thoracic and lumbar fractures. J Orthop Trauma 2001;15:566–9. ArticlePubMed
- 29. Siebenga J, Leferink VJ, Segers MJ, et al. Treatment of traumatic thoracolumbar spine fractures: a multicenter prospective randomized study of operative versus nonsurgical treatment. Spine (Phila Pa 1976) 2006;31:2881–90. ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite