Articles
- Page Path
- HOME > J Trauma Inj > Volume 36(3); 2023 > Article
-
Original Article
Treatment results of cardiac tamponade due to thoracic trauma at Jeju Regional Trauma Center, Korea: a case series -
Jeong Woo Oh, MD1
 , Minjeong Chae, PhD2
, Minjeong Chae, PhD2 -
Journal of Trauma and Injury 2023;36(3):180-186.
DOI: https://doi.org/10.20408/jti.2022.0061
Published online: January 31, 2023
- 1,356 Views
- 55 Download
1Department of Trauma Surgery, Jeju Regional Trauma Center, Cheju Halla General Hospital, Jeju, Korea
2Department of Nursing, Chosun Nursing College, Kwangju, Korea
- Correspondence to Jeong Woo Oh, MD Department of Trauma Surgery, Jeju Regional Trauma Center, Cheju Halla General Hospital, 65 Doryeong-ro, Jeju 63127, Korea Tel +82-64-740-5000 E-mail: johjw@hanmail.net
Copyright © 2023 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- The purpose of this study was to report the treatment results of patients with traumatic cardiac tamponade after the opening of Jeju Regional Trauma Center.
-
Methods
- We analyzed the treatment outcomes of patients with traumatic cardiac tamponade who were treated at Jeju Regional Trauma Center from January 2018 to August 2022.
-
Results
- Seven patients with traumatic cardiac tamponade were treated. The male to female ratio was 1.33:1 (four male and three female patients) and the average age was 60.3±7.2 years. The mechanism of injury was blunt trauma in six cases and penetrating injury in one case. Upon arrival at the emergency department, pericardiostomy was performed in four cases, and an emergency operation was performed in six cases. Pericardiostomy alone was performed in one patient, who had cardiac tamponade due to extrapericardial suprahepatic inferior vena cava rupture. The causes of cardiac tamponade were right atrium appendage rupture in one case, right ventricle rupture in one case, inferior vena cava rupture in two cases, right atrium and left atrium rupture in one case, both atria and left ventricle rupture in one case, and intercostal artery rupture in one case. In three cases, intraoperative cardiopulmonary bypass was required. Two of the seven patients died (mortality rate, 28.5%).
-
Conclusions
- Relatively favorable treatment results were observed for traumatic cardiac tamponade patients after Jeju Regional Trauma Center was established.
- Background
- The treatment of traumatic cardiac tamponade remains a difficult problem when treating severe trauma patients [1]. In all trauma patients, the incidence of traumatic cardiac tamponade due to thoracic injury is very low (0.16%–2%), but the mortality rate is relatively high (postoperative mortality, 24%) [2]. For the successful treatment of traumatic cardiac tamponade patients, it is important to promptly transport them from the scene of the accident to an emergency center where a prompt diagnosis and surgical treatment are possible. For this, there must be appropriate medical equipment for diagnosis and treatment, and close cooperation between skilled medical team members is required [3,4].
- Objectives
- This study analyzed the electronic medical records of patients with traumatic cardiac tamponade who were treated after the establishment of Jeju Regional Trauma Center to determine their treatment results and factors affecting the treatment outcomes.
INTRODUCTION
- Ethics statement
- The study was approved by the Institutional Review Board of Cheju General Hospital (No. 2022-L04-01). The requirement for informed consent was waived due to the retrospective nature of the study.
- Study design and patients
- From January 2018 to August 2022, seven patients with traumatic cardiac tamponade were treated at Jeju Regional Trauma Center. We conducted a retrospective study based on a review of the patients’ medical records. The subjects were patients in whom cardiac tamponade was confirmed by a physical examination and imaging studies, including ultrasonography, at the time of arrival at the emergency department. Patients with confirmed cardiac tamponade who could not be resuscitated due to cardiac arrest before arriving at the emergency department were excluded from the study.
- Data collection
- We reviewed patients’ medical records and collected data related to their general characteristics. Sex, age, transport time, injury mechanism, vital signs, Glasgow Coma Scale, the Injury Severity Score (ISS), and Injury Severity Score (TRISS) were collected. Emergency medical records, operative records, and the outcomes of the intervention were reviewed to obtain data related to the operative procedure and findings, the results of treatment, and postoperative complications.
- Statistical analysis
- Statistical analyses were performed using IBM SPSS ver. 20 (IBM Corp). Descriptive statistics of the basic characteristics of patients were calculated. We examined whether there were differences in the mean scores of basic characteristics and the trauma score of patients according to whether they survived or died. The independent samples t-test was used to determine whether any variables showed significant differences between the survival and death groups.
METHODS
- From January 2018 to August 2022, nine patients were diagnosed with traumatic cardiac tamponade at Jeju Regional Trauma Center. Among them, two patients presented to the hospital in cardiac arrest although resuscitation was performed; since they did not recover, they were excluded from the analysis. Therefore, seven patients were included in the study (Table 1).
- The average age of the patients was 60.3±7.2 years, and the male to female ratio was 1.33:1. The average transport time to the emergency department after the accident was 48±26.6 minutes, and the causes of the accidents were blunt chest injury due to traffic accidents in six cases (85.7%) and a thoracic penetrating injury due to a stab wound in one case (14.3%).
- The diagnosis of traumatic cardiac tamponade in the emergency department was made on the basis of a physical examination and emergency ultrasonography (extended focused assessment with sonography for trauma [eFAST]). When the vital signs were stable, a whole-body computed tomography (CT) was performed immediately to make an accurate diagnosis. eFAST is a diagnostic test that plays an important role in the diagnosis and treatment of cardiac tamponade. If necessary, pericardiostomy can be performed under ultrasound guidance, and accompanying thoracic and abdominal injuries can also be screened. All seven patients treated at this center were diagnosed with cardiac tamponade by ultrasound examinations, and two patients underwent surgery immediately after the ultrasound examination without additional imaging tests.
- Six patients had bony thorax injuries (sternum or rib fractures), and five patients had lung injuries, including lung laceration, hemothorax, and pneumothorax. Associated injuries other than those to the chest were observed in three cases: abdominal injuries in two cases and pelvic bone fractures in one case (Table 2).
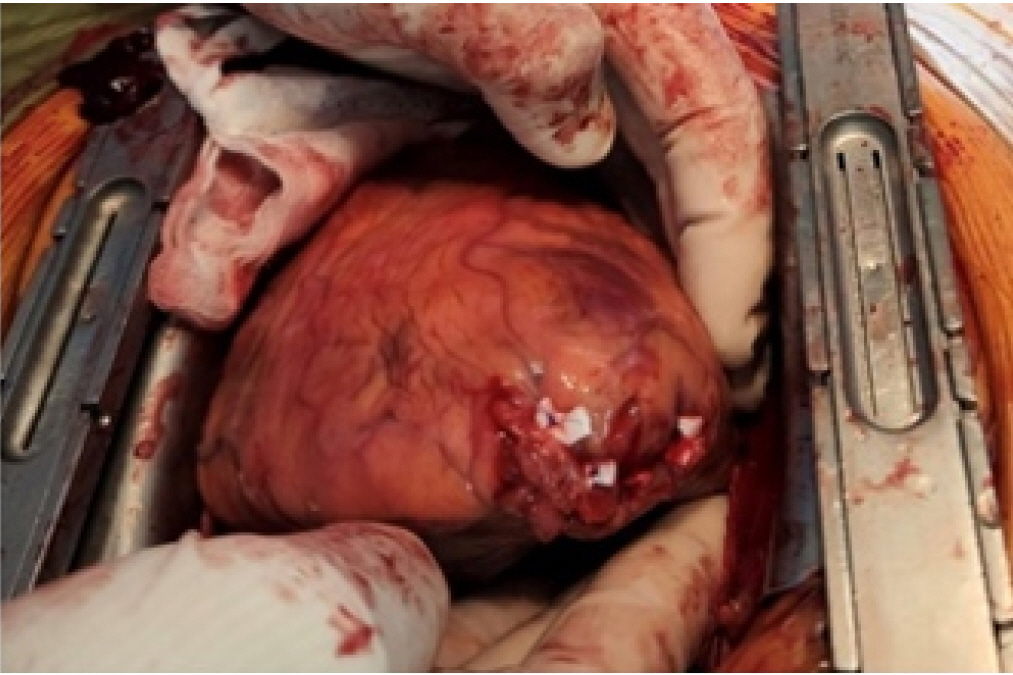
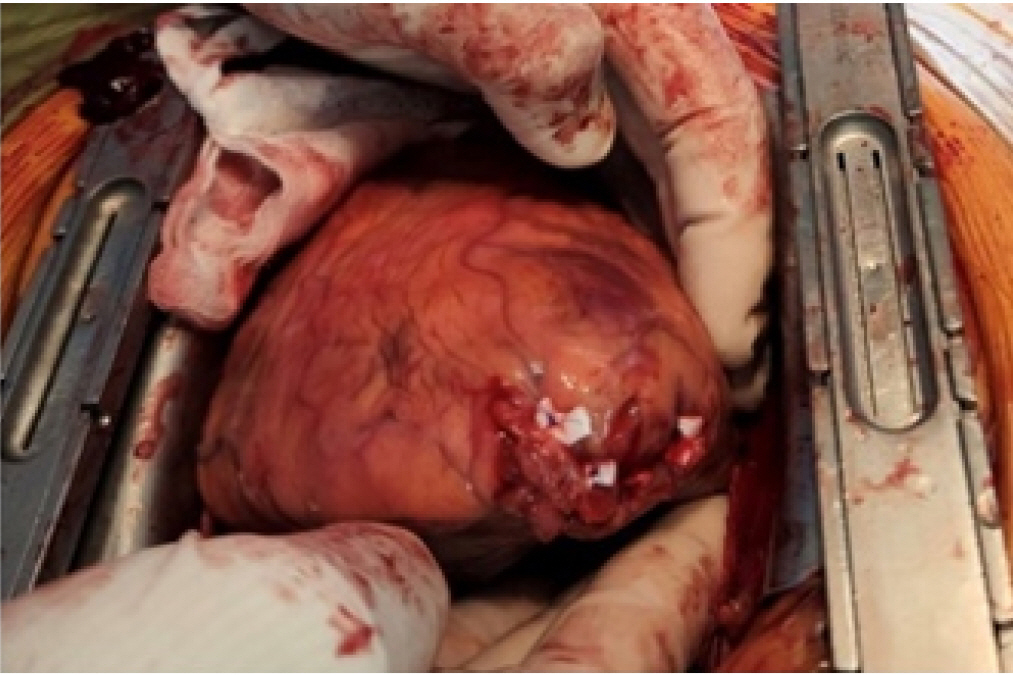
- An emergency operation was performed in six of the seven patients. Median sternotomy was performed in all operations. During surgery, extracorporeal circulation support was required in three cases, and the other cases could be sutured directly without extracorporeal circulation support (Fig. 1). In one patient, venoarterial extracorporeal membrane oxygenation (VA-ECMO; i.e., extracorporeal cardiopulmonary resuscitation [ECPR]) was applied because the blood pressure was not maintained in the emergency department before the operation. After transfer to the operation department, surgery was performed with the patient switched from VA-ECMO to extracorporeal circulation using a cardiopulmonary bypass machine.
- The cardiac and vascular injury sites identified during surgery were the right atrium in one case, inferior vena cava (IVC) in two cases, right ventricle in one case, right atrium and left atrium in one case, and right atrium, left ventricle, and IVC in one case. In patients who died, the rupture of the heart involved two or more chambers (Table 3).
- Five patients survived and were discharged, and two died, resulting in a mortality rate of 28.5%. Although there was a small number of treated patients, we did perform a statistical analysis between the survival and death groups. As a result, the ISS was significantly higher in patients who died (P=0.09) and the TRISS was significantly higher in patients who survived (P<0.001) (Table 4).
- One patient who presented to the hospital with a chest penetrating injury caused by a right anterior chest stab wound underwent surgery. At the time of arrival, the patient’s blood pressure was 78/54 mmHg and cardiac tamponade was diagnosed on eFAST. According to the operative findings, the right third rib and intercostal artery were cut, and an open wound of 1 cm was observed on the right side of the pericardium. This was a very rare case where intercostal artery bleeding flowed into the pericardium and caused cardiac tamponade (Fig. 2).
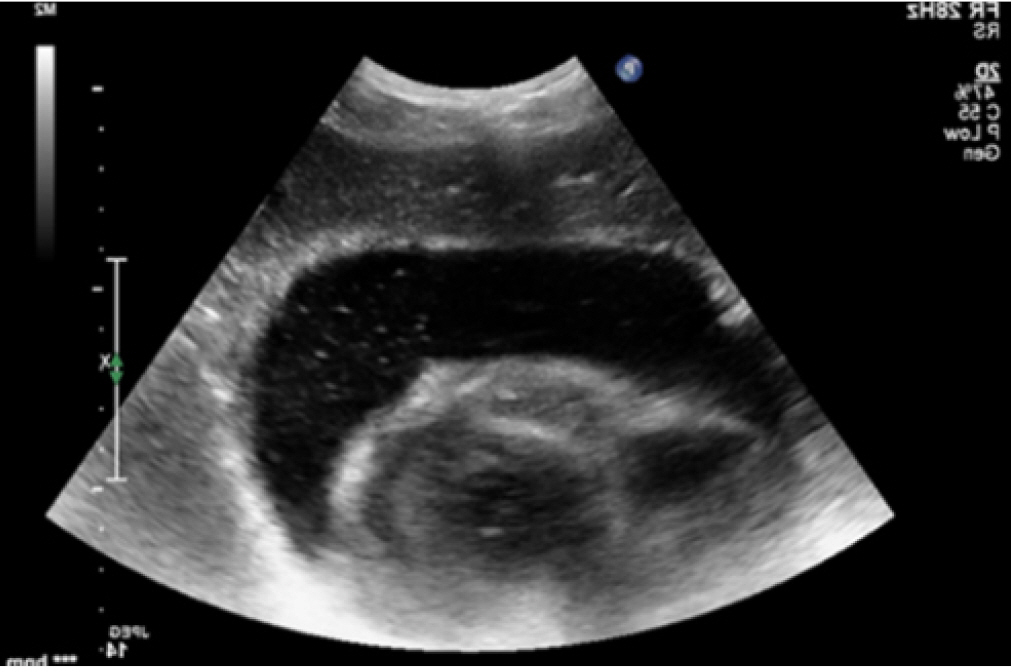
- In one patient with suprahepatic IVC rupture, treatment was possible by pericardiostomy alone without open thoracic surgery. The patient was a 60-year-old female presented to the emergency department with a blunt chest injury due to a traffic accident. At that time, her blood pressure was 67/47 mmHg, cardiac tamponade was confirmed on eFAST, and pericardiostomy was performed immediately. Enhanced chest CT showed a suprahepatic IVC rupture near the diaphragm, and a difficult operation was expected. No additional bleeding was observed after the first 300 mL of blood was drained following pericardiostomy. Then, the vital signs remained stable without any bleeding, and the pericardiostomy tube could be removed 7 days after the procedure. On the 14th day after admission, delayed cardiac tamponade (perhaps related to novel oral anticoagulant rivaroxaban use) occurred, but this was also treated with pericardiostomy, and she was discharged without any problems (Figs. 3, 4).
RESULTS
- From January 2018 to August 2022, seven traumatic cardiac tamponade patients were treated at Jeju Regional Trauma Center. Five patients survived and two patients died, resulting in a mortality rate of 28.5%. This result is similar to a 26.6% rate reported at a trauma center in Korea and a 28.6% rate reported at trauma centers abroad [5,6].
- Although the difference was not statistically significant, higher ISS and lower TRISS were found in the patients who died. These results are similar to those of previous studies [5,7].
- When comparing the anatomical locations of the damaged heart and great vessels in the surviving and deceased cases based on the surgical findings, single atrium and single ventricle ruptures were observed in the surviving cases, and multichamber damage was observed in the deceased cases. This result also aligns with those of previous studies [5,7].
- Most patients with traumatic pericardial tamponade require surgical treatment [7–10]. Among the treatment cases at Jeju Regional Trauma Center, one case of IVC rupture at the diaphragm level was treated with pericardiostomy alone without open thoracic surgery. In this case, the rupture of the IVC was at a site where compression hemostasis was possible due to the diaphragm structure and the connective tissue around the liver, and natural healing was possible. If an IVC rupture does not extend into the pericardium, the bleeding volume after pericardiostomy is less than 100 mL/hr, and if the blood pressure is stably maintained, natural healing without open thoracic surgery can be expected.
- For the effective treatment of traumatic cardiac tamponade, a rapid prediction based on clinical findings, prompt diagnosis, and surgical treatment are important [11,12]. Emergency ultrasonography can be performed immediately after the patient arrives at the hospital to diagnose cardiac tamponade, and it can also predict accompanying major abdominal and chest injuries. Pericardiostomy to relieve cardiac tamponade before open thoracic surgery can also be performed under ultrasonography. In blunt chest trauma, patients have severe soft tissue edema, subcutaneous emphysema, and a distended abdomen and pneumothorax [13,14]. These conditions reduce the accuracy of ultrasonography in blunt cardiac injury. However, repeated ultrasonography examinations can overcome these problems.
- In one case, VA-ECMO (ECPR) was applied before open thoracic surgery because the blood pressure was not maintained even after pericardiostomy. Multichamber rupture was observed, and this patient died from multiorgan dysfunction syndrome caused by massive intraoperative bleeding and postoperative low cardiac output syndrome. If a patient is hemodynamically very unstable, switching to extracorporeal circulation in the operating department after VA-ECMO (ECPR) in the emergency department may be considered [15].
- Limitations
- This study had some limitations. First, few cases of traumatic cardiac tamponade in this study; therefore, a meaningful statistical analysis was not possible. Also, this was a retrospective study conducted at a single trauma center. To obtain meaningful statistical data, we need to obtain data related to the treatment of cardiac tamponade from multiple centers over a longer period.
- Conclusions
- Over the past 4 years, after establishing Jeju Regional Trauma Center, seven patients were treated for traumatic pericardial tamponade. Five patients survived, showing a relatively favorable survival rate of 71.5%.
DISCUSSION
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
The authors did not receive any financial support for this study.
-
Data availability
Data of this study are available from the corresponding author upon reasonable request.
-
Author contributions
Conceptualization: JWO; Data curation: JWO; Formal analysis: MC; Writing–original draft: JWO; Writing–review & editing: all authors. All authors read and approved the final manuscript.
ARTICLE INFORMATION


Arrival, transport time; BP, blood pressure; PP, pulse rate; RR, respiratory rate; GCS, Glascow Coma Scale; ISS, Injury Severity Score; RTS, Revised Trauma Score; TRISS, Trauma and Injury Severity Score; ICU, intensive care unit stay time; Adm, admission day; Cx, complication; TA, traffic accident; MRF, multiple rib fracture; RA, right atrium; CPB, cardiopulmonary bypass; RAA, right atrium appendage; IVC, inferior vena cava; LV, left ventricle; VA-ECMO, venoarterial extracorporeal membrane oxygenation; LA, left atrium; MCA, middle cerebral artery; RV, right ventricle.
| Associated injury | No. of cases |
|---|---|
| Fracture of bony thorax (rib or sternum) | 6 |
| Hemothorax or hemopneumothorax | 5 |
| Lung contusion or laceration | 1 |
| Spleen rupture | 1 |
| Liver laceration | 1 |
| Pelvic bone fracture | 1 |
| Cardiac injury | Survival group (n=5) | Death group (n=2) |
|---|---|---|
| RA | 1 | 0 |
| IVC | 2 | 0 |
| RA+LA | 0 | 1 |
| RV | 1 | 0 |
| IVC+RA+LV | 0 | 1 |
| Extrapericardial vascular injury | 1 | 0 |
- 1. Teixeira PG, Inaba K, Oncel D, et al. Blunt cardiac rupture: a 5-year NTDB analysis. J Trauma 2009;67:788–91. ArticlePubMed
- 2. Yun JH, Byun JH, Kim SH, et al. Blunt traumatic cardiac rupture: single-institution experiences over 14 years. Korean J Thorac Cardiovasc Surg 2016;49:435–42. ArticlePubMedPMC
- 3. Rodrigues AJ, Furlanetti LL, Faidiga GB, Scarpelini S, Barbosa Evora PR, de Andrade Vicente WV. Penetrating cardiac injuries: a 13-year retrospective evaluation from a Brazilian trauma center. Interact Cardiovasc Thorac Surg 2005;4:212–5. ArticlePubMed
- 4. Ishida K, Kinoshita Y, Iwasa N, et al. Emergency room thoracotomy for acute traumatic cardiac tamponade caused by a blunt cardiac injury: a case report. Int J Surg Case Rep 2017;35:21–4. ArticlePubMedPMC
- 5. Lee SH, Jang MJ, Jeon YB. Blunt cardiac injuries that require operative management: a single-center 7-year experience. J Trauma Injury 2021;34:242–7. ArticlePDF
- 6. Mishra B, Gupta A, Sagar S, Singhal M, Kumar S. Traumatic cardiac injury: experience from a level-1 trauma centre. Chin J Traumatol 2016;19:333–6. ArticlePubMedPMC
- 7. Nan YY, Lu MS, Liu KS, et al. Blunt traumatic cardiac rupture: therapeutic options and outcomes. Injury 2009;40:938–45. ArticlePubMed
- 8. El-Menyar A, Al Thani H, Zarour A, Latifi R. Understanding traumatic blunt cardiac injury. Ann Card Anaesth 2012;15:287–95. ArticlePubMed
- 9. Soto JR, Murry JS, Truitt MS, Dunn EL. Penetrating cardiac injuries at a level II trauma center: a 15-year review. Am Surg 2015;81:324–5. ArticlePubMedPDF
- 10. Heus C, Mellema JJ, Giannakopoulos GF, Zuidema WP. Outcome of penetrating chest injuries in an urban level I trauma center in the Netherlands. Eur J Trauma Emerg Surg 2019;45:461–5. ArticlePubMedPDF
- 11. Hoffman L, Pierce D, Puumala S. Clinical predictors of injuries not identified by focused abdominal sonogram for trauma (FAST) examinations. J Emerg Med 2009;36:271–9. ArticlePubMed
- 12. Vance S. The FAST scan: are we improving care of the trauma patient? Ann Emerg Med 2007;49:364–6. PubMed
- 13. Hartung O, Leprince P, Deneuville M. Delayed atrial rupture after blunt chest trauma. J Trauma 1998;45:833–4. ArticlePubMed
- 14. Powell MA, Lucente FC. Diagnosis and treatment of blunt cardiac rupture. W V Med J 1997;93:64–7. PubMed
- 15. Lee N, Tang D, Jayaraman S. Penetrating cardiac trauma and the use of emergent extracorporeal membrane oxygenation and therapeutic hypothermia: when cooler heads prevail. Trauma Case Rep 2015;1:95–8. ArticlePubMedPMC
 PubReader
PubReader ePub Link
ePub Link Cite
Cite