Removal of broken syndesmotic screw with minimal bone defects in Korea: a case report
Article information

Abstract
Ankle fractures with syndesmotic injuries often require fixation, where metal screw fixation is a popular method. However, as the patient begins weight-bearing, most syndesmotic screws tend to loosen or break, and removal of such screws has been challenging for the surgeons, as the available techniques require predrilling or trephination and are associated with risks of bone damage. This study presents a case with technical tip for the removal of broken tricortical-fixed non-cannulated syndesmotic screws. It implements the generation of a small cortical window in the medial distal tibia and the use of pliers to engage the screw tip and remove through the medial side. The technique presented in the current study overcomes these limitations and facilitates minimal bone damage and reduced exposure to radiation.
INTRODUCTION
Ankle fractures often accompany syndesmotic injuries and require fixation. While various methods such as suture-button or bioabsorbable screw fixation have been used recently, metal screw fixation remains the mainstay [1]. However, as the patient begins weight-bearing, most syndesmotic screws tend to loosen or break, where intraosseous breakage is associated with higher rates of implant removal compared to that in the clear space [2]. Although previous studies have reported techniques to remove a broken syndesmotic screw [3–5], there exists limitations concerning the removal of a tricortical-fixed non-cannulated screw. Furthermore, as a case of distal tibial fracture following syndesmotic screw removal has been previously reported [6], caution is required.
Therefore, we present a technical tip for removing a broken tricortical-fixed non-cannulated syndesmotic screw. It implements the generation of a small cortical window in the medial distal tibia and the use of pliers, for minimizing bone defects.
CASE REPORT
A 20-year-old male patient presented to the outpatient clinic with a chief complaint of intermittent right ankle pain. He had undergone open reduction and internal fixation of an ankle fracture with syndesmotic screw fixation 4 weeks before the visit. He insisted that he started weight-bearing with walker boots for a few days. Physical examination showed no definite sign of swelling or tenderness at the level of the ankle joint. A plain radiograph revealed intraosseous breakage of the 3.5-mm syndesmotic screw in the distal fibula (Fig. 1A). However, the screw was within the appropriate position, and considering that it was too early to remove, the patient was recommended another 4 weeks of conservative treatment by following toe touch partial weight-bearing with walker boots.
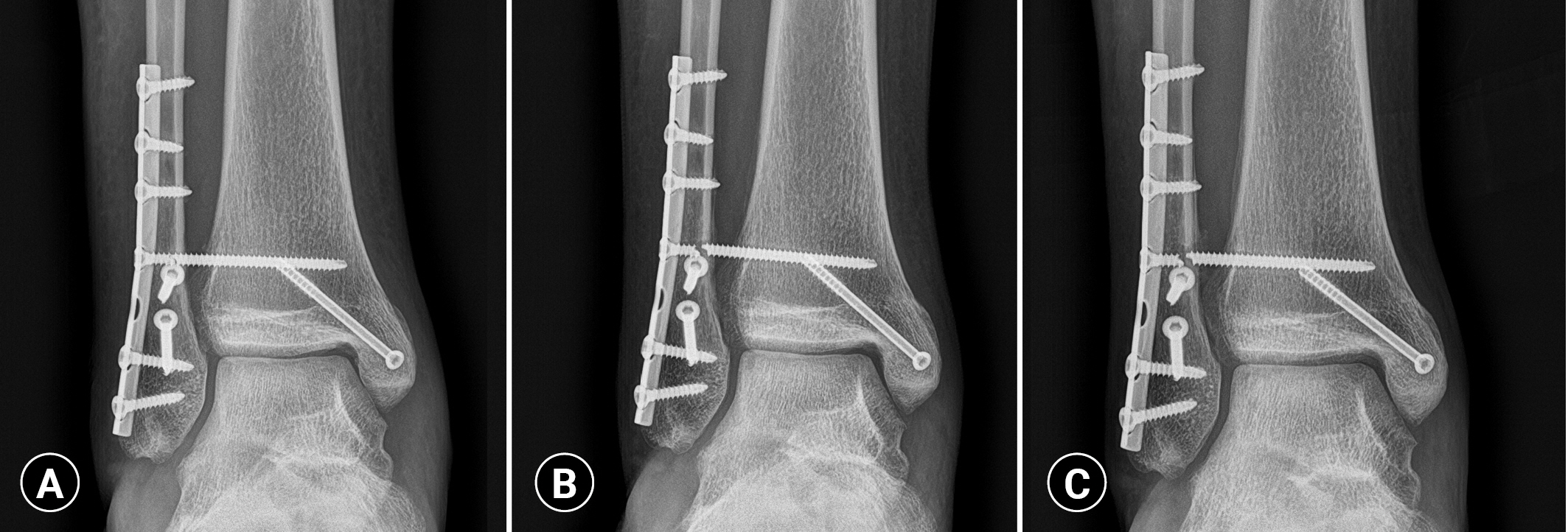
Serial radiographs following syndemostic fixation. (A) Breakage of a 3.5-mm syndesmotic screw at the intraosseous portion of fibula observed at 4 weeks postoperatively. (B) Aggravated displacement of the broken syndesmotic screw at 8 weeks postoperatively. (C) A slightly bony erosion at the broken gap observed at 12 weeks postoperatively.
Eight weeks postoperatively, the patient reported no aggravation in pain; however, a plain radiograph showed that the displacement of the broken syndesmotic screw had worsened (Fig. 1B). We decided to remove the screw 12 weeks postoperatively as previous studies reported that it takes approximately 12 weeks for the recovery of syndesmotic soft tissues, and too early removal of the screws may lead to syndesmotic diastasis [7,8]. At 12 weeks postoperatively, the plain radiograph showed a slightly bony erosion at the broken gap (Fig. 1C).
Following spinal anesthesia, the patient was placed in a supine position. Initially, the level of the broken screw tip was identified using fluoroscopy. A 2-cm to 3-cm incision was made, and careful dissection was performed to avoid any saphenous nerve and vein injury. Further, a 1×1-cm square-shaped cortical window was created with a saw, and the depth of corticotomy was calculated from the preoperative computed tomography images (Fig. 2). The tip of the broken screw was exposed when the depth of the cortical window reached 8 to 10 mm (Fig. 3A). A plier (Aesculap Inc., Center Valley, PA, USA) was used to engage the screw tip, and it was removed through the medial side by rotating in a counterclockwise direction (Fig. 3B, C). Autogenous bone grafting was performed using bones from the original tibial cortex combined with a cancellous bone chip allograft to cover the bone defect area. Subsequently, a 1-cm incision was made on the lateral side, and the remnant screw head was removed easily with a driver (Fig. 3D). The wound was closed, and an ankle brace was applied for 4 weeks postoperatively. The patient was instructed to bear a tolerable amount of weight while avoiding heavy sports and activities during those periods.
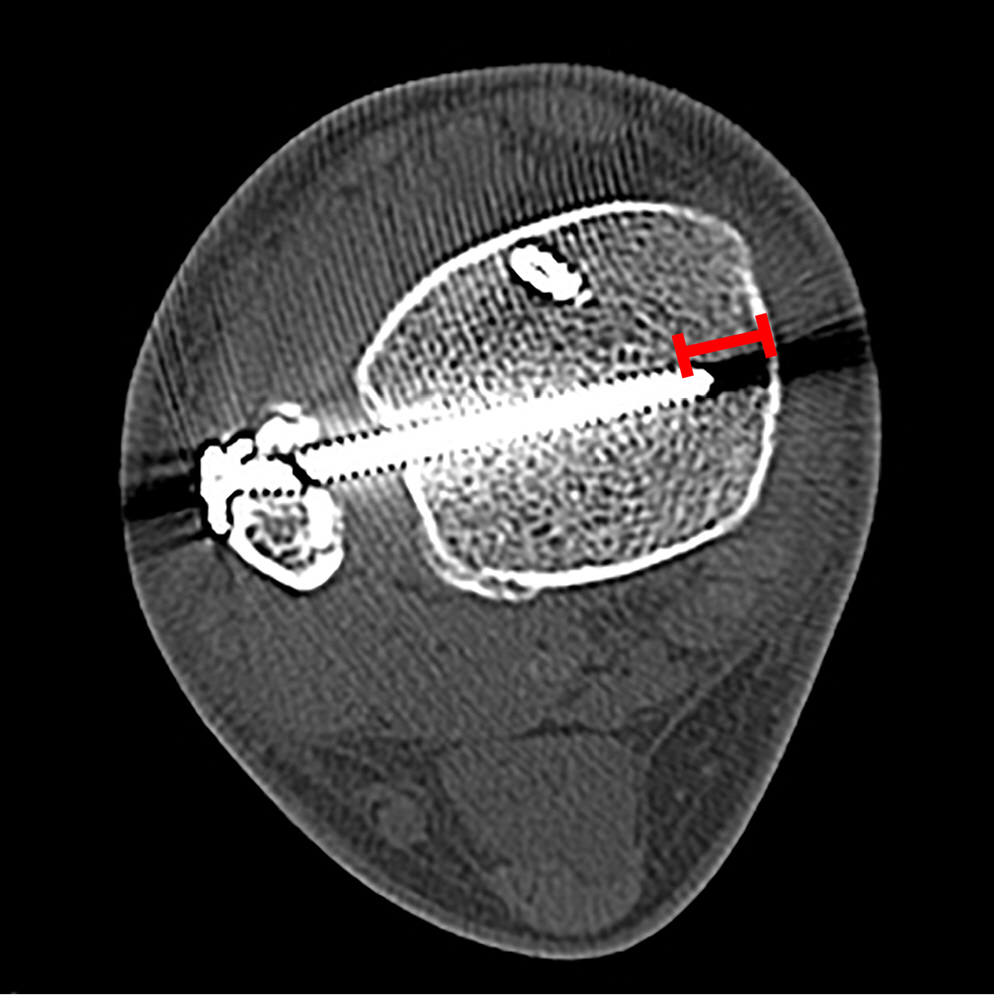
A preoperative computed tomography image used to calculate the depth (line) of corticotomy.

Description of the procedure. (A) A 1×1-cm cortical window in the medial distal tibia was created using a saw; the tip of the screw can be seen. (B) A plier was used to hold the screw tip, and (C) the screw was extracted by rotating the plier in a counterclockwise direction. (D) Image of the removed broken syndesmotic screw.
Four months postoperatively, successful consolidation of the cortical window was observed with minimal bone defects near the previous screw site (Fig. 4). At this point, the patient experienced no pain or difficulty sustaining daily activities or playing sports.

Final follow-up (4 months postoperatively). (A) Standing ankle radiograph and computed tomography of (B) coronal and (C) axial images, showing successful consolidation at the cortical window and a minimal bone defect near the previous screw site.
Ethics statement
We conducted this study in compliance with the principles of the Declaration of Helsinki. This study was approved by the Institutional Review Board of the Armed Forces Medical Command (No. AFMC-202207-HR-034-02). Written informed consent for publication of the research details and clinical images were obtained from the patient.
DISCUSSION
Although breakage of syndesmotic screws is a commonly encountered complication, their removal may be challenging for surgeons, especially a tricortical-fixed non-cannulated screws compared to quadricortical-fixed cannulated screws. A previously introduced technique necessitated predrilling of the far cortex of distal tibia during syndesmotic screw fixation while anticipating possible breakage [3]. Furthermore, impacting with a blunt instrument onto a small area of the distal fibula may exert stress. The other reported technique of hollow milling from the medial side may induce a fairly wide bone defect near the screw thread across the entire tibial width [5]. In addition, if not skilled, it is not easy to perform trephination through the two perfect circles at once, which may eventually lead to several trials, causing larger bone defects and higher radiation exposure.
Contrary to the aforementioned limitations, the technique described presently has several advantages. First, it provides direct visualization of the screw tip, which could minimize excessive bone defects. Only a small distal portion of the screw needs to be exposed, sufficient to engage with the plier. Once the screw tip is engaged with the plier and rotated in a counterclockwise direction, only a hollow area as wide as the screw thread remains. While Riedel et al. [5] demonstrated a similar technical tip of removal of screws through trephination of the entire tibial width, their postoperative radiograph showed bone defects of 1.5 to 2 times the thickness of the screw thread [5]. Furthermore, if we extend the indication of our method, the technique can also be utilized in the removal of quadricortical-fixed or cannulated syndesmotic screws. Second, additional instruments required during the screw removal, such as a saw and plier, are readily available. Third, as intraoperative fluoroscopy is only employed to check the level of the screw tip, this technique facilitates reduced radiation exposure.
Despite the advantages, there are a few limitations to this technique. First, it requires an additional corticotomy at the medial side of the distal tibia to expose the screw tip. It would be a concern if the area of bone defect is large; however, in our representative case, it was merely 5% of the total area. In addition, successful consolidation of the tibial cortex was achieved by autologous bone grafting from the original tibial cortex combined with a cancellous bone chip allograft. Second, there is a possibility of saphenous vein and nerve injury associated with the technique; however, careful dissection of structures on the medial side can reduce this risk.
We believe that the technique presented herein will be of great advantage to foot and ankle surgeons who encounter a challenging case of the broken non-cannulated syndesmotic screw within the intraosseous portion during the follow-up period.
Notes
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
The authors did not receive any financial support for this study.
Data availability
Data sharing is not applicable as no new data were created or analyzed in this study.
Author contributions
Conceptualization: MGK; Data curation: all authors; Formal analysis: all authors; Investigation: all authors; Methodology: MGK; Project administration: MGK; Visualization: MGK; Writing–original draft: MGK; Writing–review & editing: all authors.
All authors read and approved the final manuscript.