Articles
- Page Path
- HOME > J Trauma Inj > Volume 35(4); 2022 > Article
-
Case Report
Gastric necrosis after gastric artery embolization in a patient with blunt abdominal trauma: a case report -
Gil Hwan Kim, MD
 , Sung Jin Park, MD, Chan Ik Park, MD
, Sung Jin Park, MD, Chan Ik Park, MD -
Journal of Trauma and Injury 2022;35(4):287-290.
DOI: https://doi.org/10.20408/jti.2022.0054
Published online: December 20, 2022
- 1,300 Views
- 34 Download
Department of Trauma and Surgical Critical Care, Pusan National University Hospital, Busan, Korea
- Correspondence to Sung Jin Park, MD Department of Trauma and Surgical Critical Care, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea Tel: +82-51-240-7369 E-mail: psjtrauma@gmail.com
Copyright © 2022 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Gastric artery bleeding after blunt trauma is rare. In such cases, if vital signs are stable, angiographic embolization may be performed. Although gastric artery embolization is known to be safe due to its anatomical properties, complications may occur. We report a case of gastric necrosis after gastric artery embolization in a patient with blunt abdominal trauma. The 55-year-old male patient was found with gastric arterial bleeding after a traffic accident. His vital signs were stable, and gastric artery embolization was performed. Gastric necrosis was subsequently found, which was treated surgically.
- Gastric arterial bleeding due to blunt trauma is uncommon [1]. However, if diagnosis or treatment is delayed, the bleeding can progress to a massive hemorrhage and cause death. Recently, angiographic embolization (AE) has been widely used for treatment of either intraabdominal hemorrhage that occurs spontaneously or is caused by trauma [2]. In particular, AE of solid organs or upper gastrointestinal bleeding above the Treitz ligament has been performed [3]. Although gastric artery embolization (GAE) is relatively safe, it is not without complications. We describe a case of patient with blunt abdominal trauma and stomach necrosis after left GAE.
INTRODUCTION
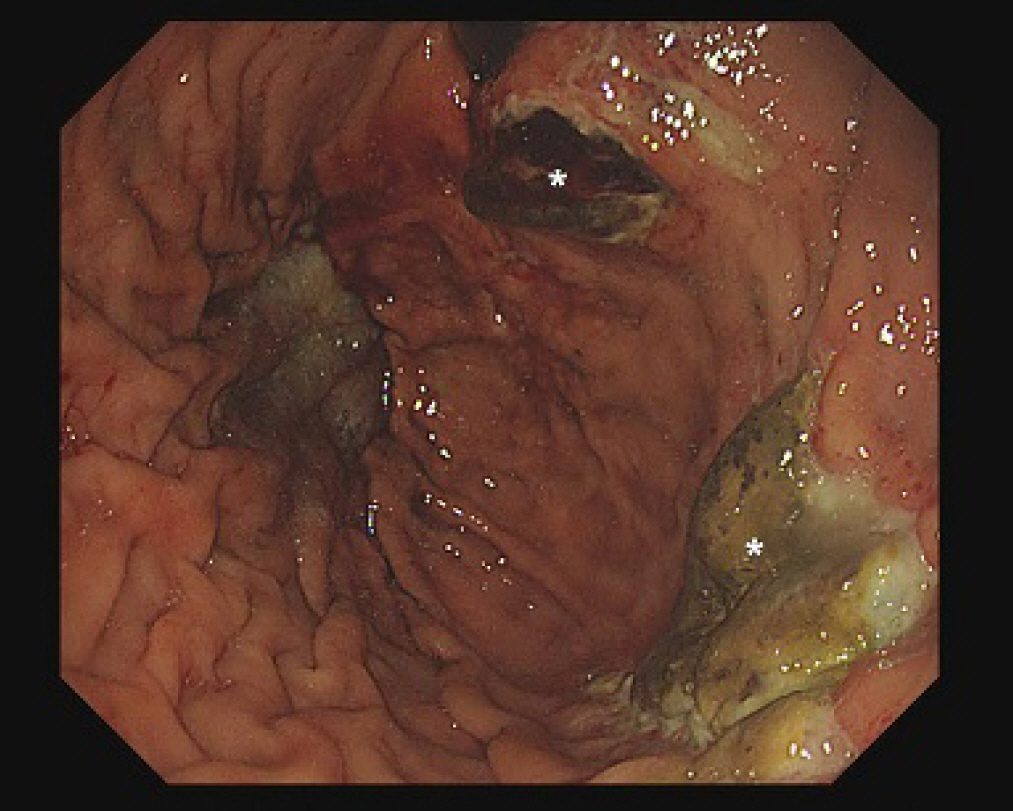
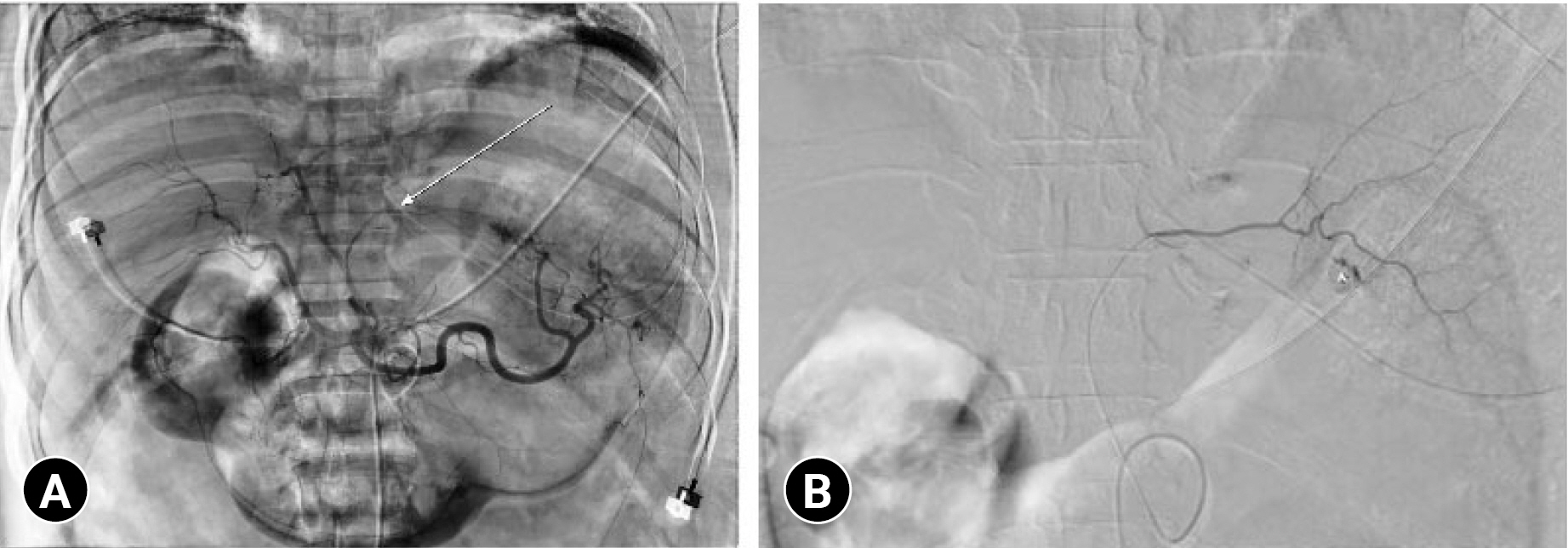
- A 55-year-old male patient with no specific medical history other than hypertension who was a truck driver was transferred to the trauma center of Pusan National University Hospital after a traffic accident with another truck. His initial vital signs were unstable, with systolic blood pressure of 60 mmHg and a Glasgow Coma Scale score of 13. Shortly after injection of 500 mL of plasma solution and 1 unit of packed red blood cells transfusion during resuscitation, his vital signs improved, and computed tomography (CT) was performed for evaluation. On contrast-enhanced abdominal CT, contrast extravasation in the hepatogastric ligament and an intramural hematoma of the stomach were observed (Fig. 1). Additionally, tiny subdural hematoma, forehead laceration, and right femur shaft fracture were accompanied; the Injury Severity Score was 27. His vital signs remained stable, and GAE was performed for hemorrhage control (Fig. 2). The patient’s mental status improved, and he was alert. Follow-up abdominal CT was performed after 1 week without the patient experiencing any abdominal symptoms. On CT, the bleeding was well controlled, and embolic material of the surrounding stomach wall was observed (Fig. 3). Intramural hematoma remained, and enhancement of gastric mucosa was reduced, so endoscopy was performed. The endoscopy showed gastric mucosal necrosis in two places (Fig. 4). We decided to perform surgical treatment. The necrotic lesions were observed grossly in the surgical field, a wedge resection of stomach while visually checking mucosa and serosa and manual repair was performed. The patient was subsequently discharged after he was able to eat without complications related to surgery.
- This study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2209-004-118). The Institutional Review Board waived the requirement to obtain informed consent.
CASE REPORT
- Compared with solid organ injuries, gastric arterial bleeding due to blunt abdominal trauma is rare. This bleeding is usually diagnosed by abdominal CT or during surgery [4]. Since intraabdominal hemorrhage is noncompressible, delayed bleeding control can lead to massive bleeding, which can be fatal [1].
- Recently, for nonvariceal upper gastrointestinal bleeding above the Treitz ligament, AE has become the preferred treatment and is performed as frequently as endoscopic hemostasis [3]. In gastric arterial bleeding other than that associated with solid organ injury in patients with abdominal trauma, GAE can be considered prior to surgical treatment if patient’s vital signs are stable [5]. Of course, if the vital signs are unstable, surgical treatment should be performed first.
- GAE can be performed relatively safely because of the anatomical characteristic of abundant blood flow around the stomach [6]. Therefore, stomach necrosis is uncommon even with GAE, so the procedure is relatively safe [7]. However, complications, such as bleeding, perforation, necrosis, vascular damage, and side effects of contrast agents, may occur [3]. In the case of trauma, especially blunt trauma, collateral blood vessels may be simultaneously damaged, which may increase the likelihood of developing stomach necrosis. Therefore, more caution is needed in patients with trauma than in those experiencing spontaneous or ulcerative bleeding. This additional caution requires that necrosis or delayed perforation be suspected and checked. A continuous physical examination is important, and follow-up CT can be performed if necessary. Even knowing that complications can occur, they are often overlooked if there are no symptoms or specific findings in the physical examination and laboratory tests. In this case, the patient had no abnormal findings on abdominal examination and laboratory tests, but mucosal injury was suspected on the initial CT, so follow-up CT and endoscopy were performed. Fortunately, his stomach necrosis was found, and surgical treatment was possible. Although necrosis can be due to direct trauma, in this case, necrosis was observed in two different places, and considering the surrounding embolic material on CT images, we judged the necrosis to have been caused by the previous embolization. As this case illustrates, in cases of partial necrosis of the stomach, there may be no abnormal findings, such as patient symptoms or in laboratory tests, so endoscopic evaluation might be required. If stomach necrosis is detected, surgical treatment should be considered, as in our case.
- GAE is considered less invasive than surgical treatment and safe, so it is widely used for bleeding control [8]. However, the possibility of complications should always be kept in mind and if there is even the slightest suspicion, an active evaluation is strongly recommended.
DISCUSSION
-
Ethical statements
This study was approved by the Institutional Review Board of Pusan National University Hospital (No. 2209-004-118). The Institutional Review Board waived the requirement to obtain informed consent.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
This work was supported by a clinical research grant from Pusan National University Hospital in 2022.
-
Author contributions
Conceptualization: all authors; Data curation: GHK; Investigation: SJP; Project administration: SJP; Visualization: CIP; Writing–original draft: GHK; Writing–review & editing: all authors.
All authors read and approved the final manuscript.
ARTICLE INFORMATION



- 1. Noh D, Mun YS. Post-traumatic pseudoaneurysms of the left gastric artery: a case report. Trauma Case Rep 2018;19:1–6. ArticlePubMedPMC
- 2. Velmahos GC, Toutouzas KG, Vassiliu P, et al. A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma 2002;53:303–8. ArticlePubMed
- 3. Shin JH. Recent update of embolization of upper gastrointestinal tract bleeding. Korean J Radiol 2012;13(Suppl 1):S31–9. ArticlePubMedPMC
- 4. Nissim L, Diven C, Braun A. Embolization of left gastric artery pseudoaneurysm after blunt trauma. Imaging Med 2017;9:15–7.
- 5. Varela JE, Salzman SL, Owens C, Doherty JC, Fishman D, Merlotti G. Angiographic embolization of a left gastric artery pseudoaneurysm after blunt abdominal trauma. J Trauma 2006;60:1350–2. ArticlePubMed
- 6. Loffroy R, Favelier S, Pottecher P, et al. Transcatheter arterial embolization for acute nonvariceal upper gastrointestinal bleeding: indications, techniques and outcomes. Diagn Interv Imaging 2015;96:731–44. ArticlePubMed
- 7. Delgado A, Patel Y, Israel T, Ismail N, Weaver J. Gastric necrosis and perforation following treatment of Dieulafoy's lesion with embolization of multiple gastric arteries: a case report. SAGE Open Med Case Rep 2022;10:2050313X221097260. ArticlePubMedPMCPDF
- 8. Nouri Y, Shin JH, Ko HK, Kim JW, Yoon HK. Embolization of procedure-related upper gastrointestinal bleeding. Int J Gastrointest Interv 2019;8:63–9. Article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite