Effect of trauma center operation on emergency care and clinical outcomes in patients with traumatic brain injury
Article information

Abstract
Purpose
Traumatic brain injury (TBI) directly affects the survival of patients and can cause long-term sequelae. The purpose of our study was to investigate whether the operation of a trauma center in a single tertiary general hospital has improved emergency care and clinical outcomes for patients with TBI.
Methods
The participants of this study were all TBI patients, patients with isolated TBI, and patients with TBI who underwent surgery within 24 hours, who visited our level 1 trauma center from March 1, 2012 to February 28, 2020. Patients were divided into two groups: patients who visited before and after the operation of the trauma center. A comparative analysis was conducted. Differences in detailed emergency care time, hospital stay, and clinical outcomes were investigated in this study.
Results
On comparing the entire TBI patient population via dividing them into the aforementioned two groups, the following results were found in the group of patients who visited the hospital after the operation of the trauma center: an increased number of patients with a good functional prognosis (P<0.001 and P=0.002, respectively), an increased number of surviving discharges (P<0.001 and P<0.001, respectively), and a reduction in overall emergency care time (P<0.05, for all item values). However, no significant differences existed in the length of intensive care unit stay, ventilator days, and total length of stay for TBI patients who visited the hospital before and after the operation of the trauma center.
Conclusions
The findings confirmed that overall TBI patients and patients with isolated brain injury had improved treatment results and emergency care through the operation of a trauma center in a tertiary general hospital.
INTRODUCTION
In Korea, trauma is the fourth leading cause of death and the most common cause of death for people under 40 years of age. Transportation accidents are the third leading cause of death among adolescents and young adults aged 10 to 39 years [1]. In addition, based on the Statistical Yearbook of the National Emergency Medical Center, as of December 31, 2020, 34,318 trauma patients visited 17 medical institutions designated as regional trauma centers in Korea. The most frequent anatomical sites that received treatment were the head and neck (68.1%) [2]. This finding suggests that patients with head injury account for a large proportion of patients treated at trauma centers. As such, traumatic brain injury (TBI) is a disease that can pose a significant threat to life and has a high possibility of causing life-long functional sequelae after an accident [3].
The development of the trauma care system, which started in developed countries such as the United States and Canada, has contributed to reducing preventable trauma deaths and increasing the survival rate of trauma patients. Moreover, based on previous studies, the importance of specialized trauma teams and trauma centers in charge of treating patients with severe trauma is understood, and the positive effects of trauma centers and trauma teams on overall trauma patient treatment outcomes have been demonstrated [4–6].
Interest in treating trauma patients has increased in Korea; therefore, regional trauma centers have been opened and operating since 2012, and, partially because of these efforts, the preventable mortality rate of patients with severe trauma is on the decline [7]. Patients with TBI have an increased survival rate when treated at trauma centers, compared to nontrauma centers [8]. However, in Korea, the effect of operating a regional trauma center on patients with TBI remains unknown. Therefore, in this study, we aimed to investigate how the operation of a trauma center affects the emergency treatment process and outcomes of patients with TBI.
METHODS
Ethical statement
This study was approved by the Institutional Review Board Wonju Severance Christian Hospital (No. 2022-0441-001). Informed consent was waived due to the retrospective nature of the study.
Study design
This study featured an observational cohort design and prospective data collection. From March 1, 2012 to February 28, 2021, among trauma patients who visited a regional trauma center, the patients who were issued an injury code related to TBI were set as the population, and the data were collected retrospectively. To compare differences in patient care, based on the operation of the trauma centers, patients were categorized into two groups according to the admission date: (1) the before trauma center group, comprising patients admitted between March 2012 and December 2014 and (2) the after trauma center group, comprising patients admitted between January 2015 and February 2021. The inclusion criteria were patients with traumatic head injuries of at least 2 points on the Abbreviated Injury Scale (AIS) and who visited the emergency department within 24 hours after the accident. Patients with head trauma who were transferred from the emergency department to another hospital were excluded because their prognosis was unknown.
The data were obtained from electronic medical records, the National Emergency Department Information System (NEDIS), and the Korean Trauma Data Bank (KTDB). The NEDIS and KTDB were developed to serve as national data repositories managed by the Korean government. Level I trauma centers are required to register with the NEDIS and KTDB. To know the basic characteristics of the patients, the following were investigated: age, sex, history, visit route, visit method, accident mechanism, and time from accident occurrence until the emergency department visit. In addition, among the clinical data, the following were also investigated immediately after the emergency department visit: consciousness level, pupil reflex, pupil size, Glasgow Coma Scale (GCS) total score, head and neck AIS, and Injury Severity Score (ISS) items. Among these, patients with incorrect or missing values were excluded from the analysis.
Study outcome
The study’s primary outcome was the difference in disability and mortality between the two groups. The Glasgow Outcome Scale (GOS) was checked on discharge to determine the patients’ disability rate. A patient’s mortality was confirmed, based on the patient’s discharge date. For the secondary outcome, we attempted to investigate the time elements related to emergency care and length of stay. Time elements related to care included the time from the emergency department visit until the decision to activate the trauma team, the time from the emergency department visit until the involvement of the neurosurgeon, the time from the emergency department visit until the neurosurgeon’s first prescription, the time from the emergency department visit until undergoing a head computed tomography (CT) scan, the time from the emergency department visit until the issuance of the inpatient admission, the time from the emergency department visit until the ward admission, and the time from the emergency department visit until entering the operating room. Our hospital had been operating a trauma team before the trauma center was opened; therefore, comparing differences in activation time of the trauma team before and after the opening of the trauma center was possible. Neurosurgeon care was defined as the care administered when the trauma team’s on-call neurosurgeon arrived at the emergency department and left a medical record. In the situation in which patients visiting the hospital had head CT data obtained at another hospital, the head CT scan time data were not included. In addition, the ventilator days of patients and the length of stay in the hospital or the intensive care unit (ICU) were checked.
Statistical analysis
The difference in injury severity between the two groups (i.e., before and after the operation of the trauma center) was adjusted through propensity score matching for the entire TBI patient group, the isolated TBI patient group, and the isolated TBI patient group who underwent surgery within 24 hours. The propensity score was estimated using logistic regression, and propensity score matching was conducted in the caliper 0.2 to 1:1 ratio for the after trauma center group, based on the covariates and the calculated propensity score. Continuous variables were compared in the form of the mean±standard deviation, using the Student t-test and chi-square test. Fisher exact test was used, as appropriate, for the categorical variables. A P-value of less than 0.05 was interpreted as statistically significant. Statistical analysis was conducted using IBM SPSS ver. 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The total number of patients with TBI enrolled in the study was 3,339. After conducting propensity score matching in a 1:1 ratio, 775 patients were in the before trauma center group and 775 patients were in the after trauma center group (Fig. 1).
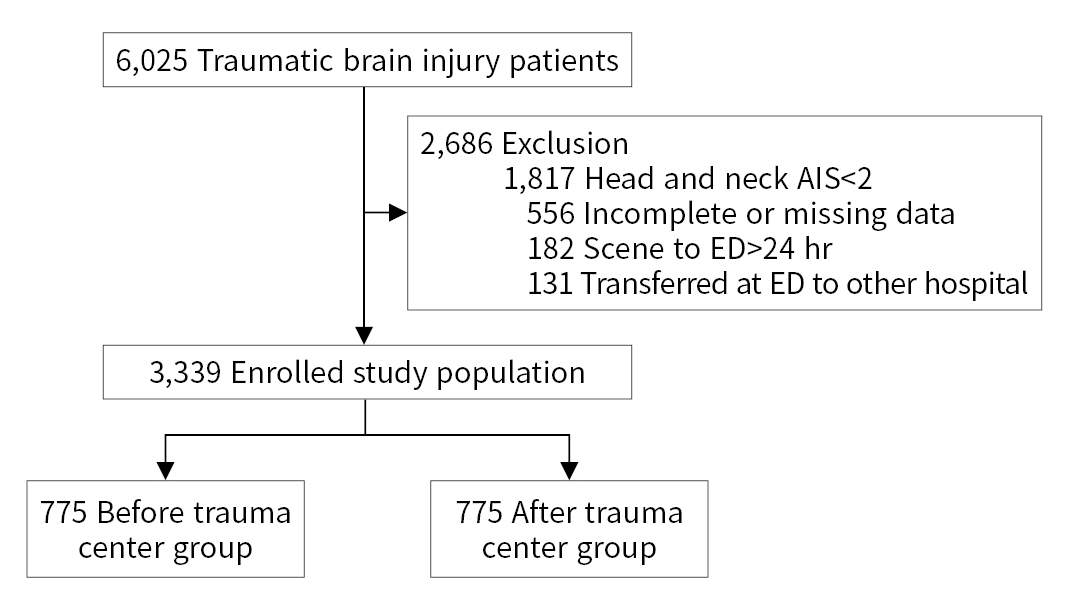
Study flowchart detailing the selection of traumatic brain injury patients in our facility. AIS, Abbreviated Injury Score; ED, emergency department.
The mean age, sex, transport route, and mechanism of injury did not differ between the two groups (Table 1). With regard to transportation, the number of patients transferred to emergency medical services was higher in the after trauma center group than in the before trauma center group, but the number of patients who visited by themselves such as by car was decreased in the after trauma center group (P=0.014). The GCS score, ISS score, AIS score, the response on arrival at the emergency department, the presence or absence of pupil reflexes in the right and left eyes, and the surgery performed on the patients were not significantly different between the two groups. However, the proportion of subdural hemorrhage patients has increased since the operation of trauma centers, which can be interpreted as an increase in the number of transfer cases of patients with TBI who are considered as requiring urgent surgery at other hospitals.

Demographic characteristics of the patients with traumatic brain injury (n=1,550)
When comparing the clinical results between the two groups, the posttrauma center group had more patients with good recovery, based on GOS score at discharge, and more surviving patients than did the before trauma center group (P<0.001 and P<0.001, respectively) (Table 2). In the after trauma center group, the time from the patient’s visit to the emergency department until the activation of the trauma team, the time until seeing a neurosurgeon, the time until undergoing a head CT scan, the time until the issuance of inpatient admission, the time to hospitalization, and the time until entering the operating room were all decreased (P=0.001, P<0.001, P<0.001, P=0.020, P<0.001, P<0.01, and P=0.030, respectively). However, differences in ICU stay, ventilator days, and the total ICU stay between the two groups were not statistically significant. In addition, no difference existed between the two groups in the time from the occurrence of an injury until the emergency department visit and the ISS score.

Clinical outcomes of before and after trauma center groups (n=1,550)
The subgroup analysis of patients with isolated TBI with an AIS score of ≤2 in areas other than the head and neck area revealed that 621 patients visited before the operation of the trauma center, and 605 patients visited after. In the after trauma center group, the number of patients with a good recovery increased (P=0.002). The proportion of survivors was increased in the after trauma center group (P<0.001), compared to the before trauma center group (Table 3). All factors related to treatment time also decreased statistically significantly. No difference existed between the before trauma center and after trauma center groups in ICU stay and ventilator days (P=0.647 and P=0.302, respectively), but the total length of stay decreased slightly in the after trauma center group (P=0.013).
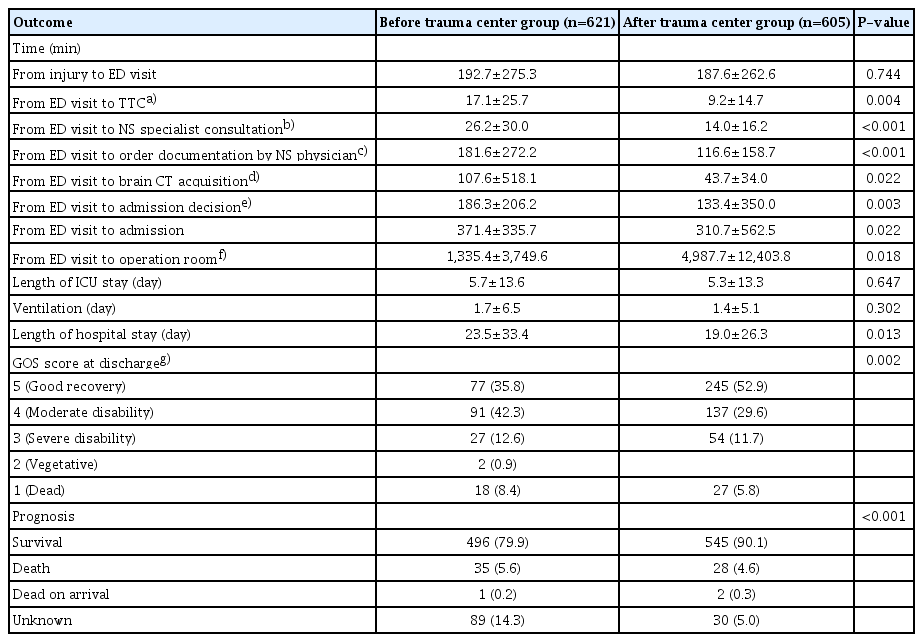
Clinical outcomes of before and after trauma center groups except for patients with area other than the head AIS≤2 (n=1,226)
Finally, a subgroup analysis of patients with isolated TBI who underwent surgery within 24 hours of visiting the emergency department was conducted (Table 4). No difference existed in the severity in the before trauma center and after trauma center groups, based on the ISS (20.7±7.7 vs. 20.7±7.2, P=0.987). Contrary to previous results, the before trauma center and after trauma center groups had no significant difference in the GOS score at discharge and survival at discharge (P=0.197 and P=0.444, respectively). No differences existed between the two groups in ICU stay, number of days on a ventilator, and length of stay (P=0.329, P=0.167, and P=0.426, respectively).

Clinical outcomes of before and after trauma center groups except for patients with area other than the head AIS≤2 and surgery done within 24 hours (n=180)
In the time items related to emergency care, the time from visiting the emergency department until receiving a prescription from a neurosurgeon and the time taken to make the decision to be hospitalized were decreased in the after trauma center group (P=0.001 and P=0.001, respectively), but no difference existed otherwise.
DISCUSSION
The purpose of our study was to investigate whether the operation of a trauma center in a single tertiary general hospital has improved emergency care and clinical outcomes of patients with TBI. Our findings confirmed that the establishment of trauma centers has had a beneficial effect on treatment results and the emergency care of patients with traumatic brain injuries. We believe this study is the first study in Korea to confirm the effect of establishing trauma centers on patients with TBIs.
In previous studies, age, GCS, pupil reflex, and CT findings were strong predictors of treatment outcomes in patients with TBI [9]. In our study, propensity score matching was conducted so that no statistical difference existed in these baseline characteristics in the groups before and after the operation of the trauma center. Moreover, we identified an improvement in the disability and survival rates of patients with a TBI in the after trauma center group, even with the selection bias reduced through propensity score matching. Some reports have shown that patients with severe TBI treated at a level I trauma center had better survival rates and clinical outcomes than patients treated at a lower level trauma center [10,11]. Our study also showed that the survival rate and the functional prognosis of patients with TBI improved after the operation of the trauma center, which was consistent with results reported in previous study [4]. The difference in prognosis was not statistically significant between the two groups in patients with isolated TBI who underwent surgery 24 hours after visiting the emergency department, although the proportion of patients who survived and were discharged after the operation of the trauma center was higher than that before the operation of the trauma center. The proportion slightly increased (before, 75.6% vs. after, 80.0%).
One purpose of this study was to investigate in more detail how a trauma center affects the emergency treatment process of trauma patients via the analysis of time items related to emergency treatment. It was observed that the time from the visit of the trauma patient until the activation of the trauma team and the treatment and prescription by the neurosurgeon was faster after the operation of the trauma center, which is presumedly because of improvement in the trauma team activation system. In our hospital, after starting the trauma center, the trauma care system was improved in such a way that surgical specialists from each department, including neurosurgeons belonging to the trauma team, could quickly treat patients and make treatment plans immediately after visiting trauma patients in the emergency department. As a result, discussions among specialists regarding the initial diagnosis and treatment plan of trauma patients have become active, and the actual treatment start time seems to have been shortened.
An accepted fact is that patients with TBI need a head CT scan as immediately as possible to confirm the degree of brain damage and to determine whether the lesion requires surgical treatment [12]. Furthermore, a CT scan significantly shortens the time spent in the emergency department, including the time for interventions such as surgery [13,14]. In addition, based on the results of a previous study, the mortality rate in patients with TBI aged 70 years or older increases in proportion to a delay in brain injury diagnosis [13]. To reduce the waiting time for CT scans, a CT scan room for trauma patients was newly established in the trauma center. In addition, this CT imaging room is operated with the highest priority for trauma patients visiting the emergency department and patients admitted to the trauma ward via cooperation with the hospital’s computer system and radiology department. Based on the results of one study, the reduction in CT waiting time for trauma patients after visiting a trauma center may reflect the development of facilities and systems for trauma patient treatment [15]. In addition, the time from visiting the emergency department until a hospital admission letter was issued and the length of hospitalization were shortened via establishing a ward dedicated to trauma patients.
However, no significant difference existed between the two groups in the length of ICU stay, number of days on a ventilator, and the length of hospital stay. Nevertheless, one reason that the operation of a trauma center improved the overall survival rate and the functional prognosis of patients with TBI was that the waiting time until the hospitalization of trauma patients was shortened by the establishment of a general ward and an ICU exclusively for trauma patients. This situation has made it possible to provide early overall monitoring and high-quality care for trauma patients. In general, patients with severe TBI require professional care such as real-time intracranial pressure monitoring, and cerebral perfusion pressure management, in addition to the monitoring conducted in the ICU [12].
The survival rate of patients with severe TBI requiring urgent surgical intervention is time-dependent [16]. However, in this study, survival rates did not differ between the groups of patients who underwent surgery within 24 hours before and after the opening of the trauma center. One of the main reasons for this result is the failure to effectively reduce the time from the emergency department visit to the operating room. This reflects one problem of the head injury-treatment system at this trauma center; therefore, robust quality management is required to improve the prognosis of patients with life-threatening head injuries who require surgery within 24 hours.
This study had several limitations. First, in this study, factors influencing the prognosis of patients with TBI after the operation of the trauma center were primarily associated with the time factor. Therefore, additional research is warranted because surgery or ICU treatment also affects the prognosis of patients with TBI. Second, the clinical results comparing the isolated TBI patient group who underwent surgery 24 hours after visiting the emergency department included 180 of 3,339 study participants who met the aforementioned criteria. Thus, the sample size was small. Therefore, future multicenter studies should be considered. Third, many values were missing in the data related to trauma patients before the operation of the trauma center, primarily until early 2013. Therefore, care should be taken in interpreting the results.
In this study, the survival rate was increased and a good recovery rate in the GOS score was higher in the after trauma center group than in the before trauma center group. In addition, the emergency treatment time for patients with TBI who visited the hospital was significantly reduced through the operation of the trauma center. However, the survival and disability rates for patients who underwent brain surgery within 24 hours did not improve. Future studies should focus on finding ways to improve the prognosis of patients with TBI who require surgical treatment within a short time in this regard.
Notes
Ethical statements
This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (No. 2022-0441-001). Informed consent was waived due to the retrospective nature of the study.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
None.
Author contributions
Conceptualization: HKK, KHL, OHK; Data curation: HKK, YSL, WJJ, HK, OHK; Formal analysis: HKK, KHL, YSC, KCC, SOH, OHK; Methodology: HK, KHL, SOH; Visualization: KHL, OHK; Writing–original draft: HKK, YSL, WJJ; Writing–review & editing: all authors. All authors read and approved the final manuscript.
Acknowledgements
The authors thank ChanYoung Kang, BS (Wonju Severance Christian Hospital) for his assistance in preparing the manuscript.