Outcomes of open neck injuries
Article information

Abstract
Purpose
The neck is a particularly critical region for penetrating injuries due to the close proximity of the trachea, esophagus, blood vessels, and the spinal cord. An open neck injury has the potential for serious morbidity and mortality. The purpose of this study is to evaluate the assessment and management of open neck injuries.
Methods
In this retrospective study, open neck injury patients who were admitted to the Trauma Center of Daejeon Eulji Medical Center, Eulji University between December 2015 and December 2017 were analyzed for epidemiology, the mechanism of trauma, the injured organ, complications, and mortality.
Results
Thirty-two patients presented with open neck injuries. All patients underwent computed tomographic angiography to evaluate their injuries once their vital signs stabilized. Among these patients, 27 required surgical treatment. The most commonly injured organ was the airway. There were five deaths, and the main cause of death was bleeding. Mortality was associated with the initial systolic blood pressure at the hospital and Glasgow Coma Scale.
Conclusions
Mortality from open neck injuries was associated with initial systolic blood pressure at the hospital and Glasgow Coma Scale.
INTRODUCTION
The neck, which is located between the head and the torso, contains vital structures including the trachea, carotid arteries, and spinal cord. While relatively uncommon in comparison to other parts of the body, the potential morbidity of penetrating neck trauma is apparent, due to the high density of vital structures confined to a relatively small and poorly protected area [1]. Although penetrating neck injuries were estimated to comprise 10% of all trauma patients, the overall mortality rates were estimated to be between 3% and 6%, most commonly as a result of injury to vascular structures and hemorrhage [2].
The successful management of penetrating neck injuries depends on a clear understanding of the anatomy of the neck [3]. Anatomically, the neck can be divided into three major zones, as presented by Monson et al. [4] in 1969. Using the classification of the neck into three zones makes the initial assessment and management easier, including surgical exploration and hemorrhage control. Zone I extends from the clavicle to the cricoid cartilage, zone II extends from the cricoid cartilage to the mandibular angle, and zone III extends from the mandibular angle to the base of the skull. In zone II, the carotid arteries, jugular veins, larynx, esophagus, trachea, thyroid, and nerves gather.
This study attempted to identify the factors associated with survival in patients with open neck injuries and to characterize the outcomes of penetrating neck injuries.
METHODS
This study was approved by the Ethics Committee of Daejeon Eulji Medical Center, Eulji Univeristy. Written informed consent was not necessary due to the retrospective nature of the study. From January 2015 to December 2017, we studied neck trauma cases at the Trauma Center of Daejeon Eulji Medical Center. We included patients with neck injuries and excluded those with head, torso, and extremity injuries. All relevant patients were enrolled in this retrospective study. All medical records and operative notes were reviewed.
Descriptive statistics are expressed as mean±standard deviation, unless otherwise specified. Continuous variables were compared using the Student t-test and the Mann-Whitney U-test, and categorical variables were compared using the chi-square test. Multiple logistic regression analysis was used to evaluate the risk factors for mortality from injury by estimating the corresponding odds ratios. All P-values of less than 0.05 were considered to indicate statistical significance. Statistical analysis was performed using IBM SPSS ver. 26.0 (IBM Corp., Armonk, NY, USA).
RESULTS
In this study, 6,183 patients presented to our hospital over a 3-year period, of whom 32 had open neck injuries. The study group comprised 23 male patients and nine female patients with a mean age of 50.2 years (Table 1). The injury mechanisms included 19 penetrating injuries and 13 blunt injuries. The causes of the injuries were accidents (19 patients), attempted suicide (10 patients), or attempted homicide (three patients) (Table 1).
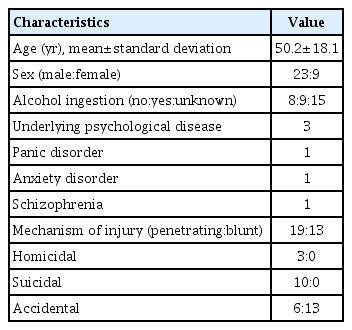
Patient characteristics
Twenty-six patients underwent computed tomographic angiography (CTA) to evaluate their injuries. Twenty-seven patients received surgical treatment once their vital signs stabilized. The damaged structures are listed in Table 2. The most commonly injured organ was the airway (eight cases) (Table 2).
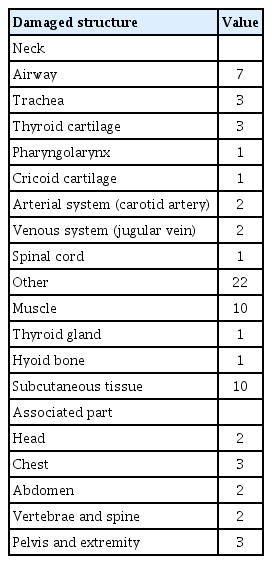
Damaged anatomical structures
The average time to rescue team arrival in the field was 45.7 minutes. The mean systolic blood pressure (SBP) in the field was 107.5 mmHg. Three patients received cardiopulmonary resuscitation in the field and during transfer to the hospital (Table 3). The average transfer time to the hospital was 37.7 minutes. The initial mean SBP at the hospital was 101.8 mmHg, and four patients received cardiopulmonary resuscitation at the hospital, including three patients who received prehospital cardiopulmonary resuscitation (Table 3). Six patients received a transfusion, and 4 units of red blood cells were transfused on average (Table 3). Table 3 shows the Glasgow Coma Scale (GCS) at the hospital.
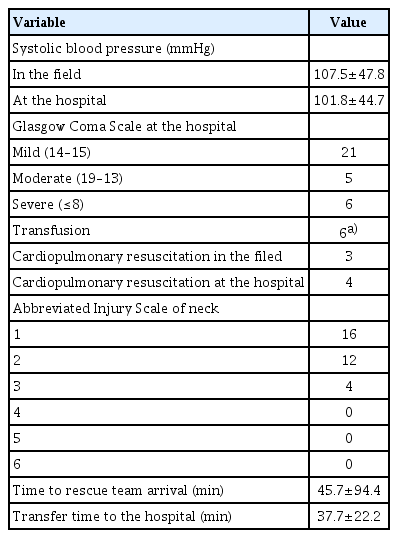
Transfer time, vital signs, and Abbreviated Injury Scale of the patients
Twenty-seven patients required surgical treatment, consisting of primary repair and temporary tracheostomy (Table 4). The average hospital stay was 15.7 days (Table 4). There were no complications, such as wound infection, pneumonia, or sepsis. There were five deaths (mortality rate, 15.6%). The causes of death were bleeding (three patients), acute drug intoxication from herbicide (one patient), and neurologic shock from spinal cord injury (one patient) (Table 4). The average time to rescue team arrival in the field and the average transfer time to the hospital were shorter in cases of mortality than in those of nonmortality (Table 5). There were differences in SBP and the GCS between the mortality and nonmortality groups (Table 5). Mortality was associated with initial SBP at the hospital and GCS (P<0.05) (Table 6).
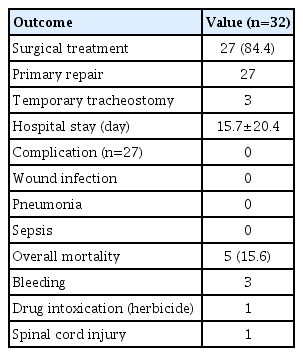
Patient outcomes
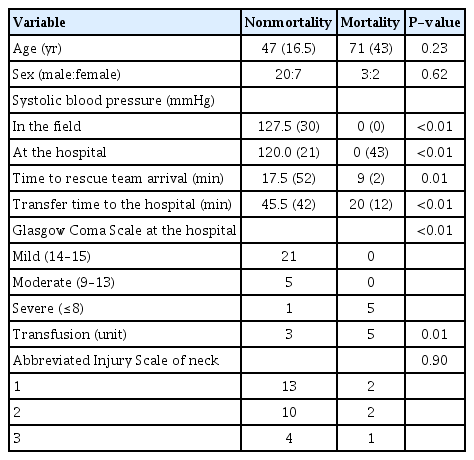
Comparison of nonmortality and mortality cases
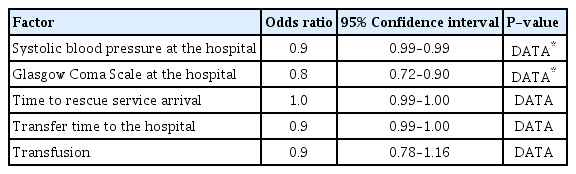
Factors influencing mortality using multiple logistic regression
DISCUSSION
In our study, mortality was associated with initial SBP and GCS at the hospital. The neck is a particularly critical region for penetrating injuries due to the close proximity of the trachea, esophagus, blood vessels, and the spinal cord. Early volume resuscitation is considered essential for open neck injury patients. Aggressive fluid therapy during transfer to the hospital and in the field would help the patient, even if the damage is severe.
The initial evaluation of a trauma patient begins with the “ABCs” of trauma management: establish a secure airway, breathing/respiration, and volume resuscitation [5–7]. For our study, the mortality was associated with initial SBP and GCS at the hospital (Table 6). The main cause of death was hypovolemia due to bleeding. SBP is considered to be the most important factor. Therefore, volume resuscitation is as important as airway management and respiration. The GCS was developed for monitoring postoperative craniotomy patients and was subsequently applied as a measure of overall physiological derangement in the trauma field. A patient’s mental status could be depressed because of hypovolemic shock [3]. Therefore, the combined use of SBP and the GCS motor scale is effective at predicting patient survival [8].
The platysma is a thin muscular sheet that surrounds the superficial fascia of the neck. It determines whether a penetrating wound of the neck is superficial or deep. The potential for injury to a vital organ exists when this structure is penetrated. The standard management is immediate surgical exploration for patients who present with signs and symptoms of shock and continuous hemorrhage from the neck wound [5]. However, all patients with active bleeding, expanding hematoma, shock, massive subcutaneous emphysema, or significant airway compromise are admitted directly to the operating room and undergo surgical exploration, regardless of the zone of injury [5,8]. Particular importance should also be placed on the airway, because bleeding within the tight compartmentalized spaces of the neck may appear quiescent externally, yet cause progressive airway compromise and eventual complete obstruction [8]. In this study, 22 patients presented with platysma penetration; significant airway or vascular injury was found in 11 patients (Table 2). Nonetheless, mandatory exploration of all neck wounds may be the best policy in an environment in which routine serial examinations are not possible [3].
CTA is generally considered the initial diagnostic method of choice for evaluating the injured organs in penetrating neck trauma [5]. A comprehensive physical examination with CTA is adequate for identifying and excluding vascular and aerodigestive injury due to penetrating neck trauma [9]. As the accuracy of CTA increases, accompanied by a careful clinical evaluation to diagnose damage to critical structures, surgical intervention or observation can be performed safely and carefully [1]. In a trauma center with experienced staff, the frequency of operations for penetrating neck wounds without structural injuries can be minimized by selective neck exploration [10,11]. In this study, all patients with stable vital signs were taken for CTA. We determined the surgical strategy based on CTA findings.
The overall mortality rate of patients with penetrating neck injuries has been estimated at between 3% to 6%, and vascular injury was the most common reason for surgery [2,12]. In this study, five patients died, with causes that included bleeding (three patients), acute drug intoxication from herbicide (one patient), and neurologic shock (one patient).
This study has several limitations. First, the single-center retrospective design of this study is its major limitation. Second, this retrospective study consisted of patients with airway injury or vascular injury. Therefore, this study group was heterogeneous. Further studies of specific injuries, such as vascular or airway injuries, seem to be necessary. Lastly, there were only 32 patients, and further studies with a larger population would be helpful. However, our data might prove to be meaningful for the prevention of death from penetrating neck injuries.
Debate continues on the assessment and management of open neck injuries. In this study, mortality from open neck injuries was associated with the initial SBP and GCS at the hospital. Further studies of open neck injuries are needed.
Notes
Ethical statements
This study was approved by the Ethics Committee of Daejeon Eulji Medical Center, Eulji Univeristy. Written informed consent was not necessary due to the retrospective nature of the study.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
The present research was supported by the research fund of Dankook University in 2020 (No. R202001203).
Author contributions
Conceptualization: DN; Data curation: all authors; Formal analysis: DN; Methodology: DN; Project administration: DN; Writing–original draft: DN; Writing–review & editing: all authors.
All authors read and approved the final manuscript.