
Articles
- Page Path
- HOME > J Trauma Inj > Volume 35(Suppl 1); 2022 > Article
-
Case Report
Extraanatomic bypass grafting in a patient with an infected femoral defect caused by a rollover accident: a case report -
Dae Sung Ma, MD1,2
 , Dong Hun Kim, MD1,3, Jae-Wook Ryu, MD2, Sung Wook Chang, MD1,2
, Dong Hun Kim, MD1,3, Jae-Wook Ryu, MD2, Sung Wook Chang, MD1,2 -
Journal of Trauma and Injury 2022;35(Suppl 1):S23-S26.
DOI: https://doi.org/10.20408/jti.2021.0005
Published online: July 21, 2022
- 1,735 Views
- 54 Download
1Trauma Center, Dankook University Hospital, Cheonan, Korea
2Department of Thoracic and Cardiovascular Surgery, Dankook University Hospital, Cheonan, Korea
3Department of Surgery, Dankook University Hospital, Cheonan, Korea
- Correspondence to: Sung Wook Chang, MD Trauma Center, Department of Thoracic and Cardiovascular Surgery, Dankook University Hospital, 201 Manghyang-ro, Dongnam-gu, Cheonan 31116, Korea Tel: +82-41-550-6195 E-mail: changsw3@naver.com
Copyright © 2022 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- A 59-year-old male patient presented to the emergency department after a tractor rollover accident. His Injury Severity Score was 41 points. He had multiple pelvic bone fractures and a left common femoral artery injury with soft tissue loss. The injured arteries with skin defect were initially managed with endarterectomy and primary repair. However, the sepsis secondary to the infection from a skin defect became uncontrolled. The infected wound developed massive hemorrhage from the repaired arteries. Supportive measures were initiated to achieve hemostasis but unsuccessful. We performed an anastomosis with a prosthetic graft from the common iliac artery to the femoral artery above the knee, avoiding the wound through the lateral side of the anterior superior iliac spine. After revascularization, the patient recovered uneventfully. An extraanatomic graft reconstruction should be considered early when the autologous vein is unsuitable.
- Vascular injuries of the extremities can result in limb loss and functional disability [1]. Furthermore, an injury to a main artery is potentially fatal, and a soft tissue defect in a lower extremity with combined skeletal and vascular injuries can be difficult to manage. This case report describes successful reconstruction using an extraanatomic graft for recurrent bleeding in the setting of a postoperative soft tissue infection complicated with skeletal and vascular injuries.
- This study was approved by the Institutional Review Board of Dankook University Hospital (No. DKUH 2022-06-29). The requirement for informed consent was waived by the Institutional Review Board.
INTRODUCTION
- A 59-year-old male patient presented to the emergency department due to a tractor rollover accident. His injury severity score was 41 points based on the injury pattern: left multiple rib fractures with hemothorax, hemoperitoneum with sigmoid colon injury, multiple pelvic bone fractures with retroperitoneal hemorrhage, and a left common femoral artery injury with 1×5-cm soft tissue loss. Bluish and mottled skin was observed below the left thigh, and pulses were clearly diminished. We performed angiography with embolization, followed by emergency exploratory surgery.
- Angiography revealed active bleeding of the left inferior gluteal and pudendal arteries, a cutoff sign for the left common femoral artery. After embolization, we explored the femoral artery and found a thrombus and ruptured atherosclerotic plaque. Thrombectomy through longitudinal arteriotomy (about 2 cm) with a Fogarty catheter was performed in the distal and proximal parts of the vessels, followed by endarterectomy and primary repair. After revascularization, gauze was packed onto the inguinal wound due to bleeding from a fractured acetabulum. We then performed an exploratory laparotomy. Segmental resection and anastomosis of the sigmoid colon, gauze packing, and temporary abdominal closure with a saline bag silo were done. The patient’s vital signs were stable on postoperative day 1, but urine output was low. Thus, continuous renal replacement therapy was applied. We closed the abdominal and inguinal wounds 2 days later.
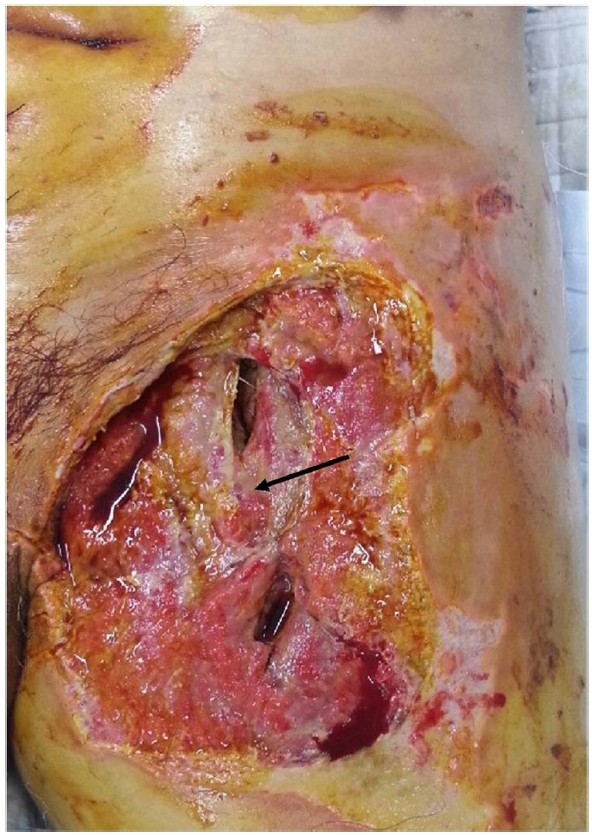
- Exudates were observed from the inguinal wound on postadmission day 6; therefore, we irrigated the wound and applied a betadine-soaked dressing. The skin defect size increased to about 20 cm, and the repaired femoral artery was exposed (Fig. 1). In addition, he developed sustained limb edema, and his condition met the severe sepsis criteria according to the 2012 Sepsis Guidelines [2]. On postadmission day 15, the exposed vascular site was checked for integrity, and vacuum-assisted closure as primary therapy in the groin was applied after covering the exposed site with adjacent tissue.
- On postadmission day 18, a massive hemorrhage occurred from the repaired femoral artery through the vacuum-assisted closure system. We repaired and reinforced the artery with a relatively fresh fasciocutaneous flap from the adjacent tissue. However, rebleeding was observed 5 days later. After bleeding control, angioplasty with a bovine patch was applied, as the previous arteriotomy edge showed friability and inflammatory changes. However, 5 days later, the sutures were reinforced with pledgets due to bleeding at the patch angioplasty site. Three days after the previous operation, recurrent bleeding resulted from inflammation and infiltration at the patch angioplasty site. Ceftriaxone as an initial empirical antibiotic was administered, a combination of piperacillin and tazobactam (Zosyn; Wyeth, Philadelphia, PA, USA) was then administered as escalation before culture, and subsequently tigecycline for multidrug-resistant Acinetobacter baumannii, colistin for tigecycline-resistant A. baumannii, and vancomycin for methicillin-resistant Staphylococcus aureus were consecutively given based on microbiological culture results from the wound. Despite the dressing and appropriate antibiotics based on culture sensitivity, the groin infection was uncontrolled and, according to the depth of involvement (Szilagyi classification) [3], it was defined as a grade III infection with vascular graft involvement. Therefore, we decided to perform the bypass grafting via an extraanatomic pathway.
- We created an anastomosis with a ringed polytetrafluoroethylene (PTFE) graft from the common iliac artery to the femoral artery above the knee on postadmission day 36. The extraanatomic graft (like a lateral femoral bypass) was placed on the lateral side of the anterior superior iliac spine to avoid cross-contamination. The final steps of the operation included local debridement, resection of the infected artery, and oversewing the deep and superficial femoral arteries.
- After revascularization, the wound was managed effectively, and the infection was controlled. Vascular computed tomography showed good graft patency (Fig. 2). A split-thickness skin graft from the right thigh was applied on postadmission day 72, and he was discharged home on postadmission day 94 without any complaints (Fig. 3).
CASE REPORT
- The optimal treatment for a patient with multiple trauma including a torso injury is difficult. In these patients, skeletal injuries complicated by vascular injuries are potentially fatal; these cases require a multidisciplinary intervention and can lead to limb loss and mortality if they are not appropriately managed. In general, after stabilization of the critical condition, the surgical procedure is based on reversing ischemia and controlling hemorrhage [4]. As a treatment for ischemia due to vascular injury, primary repair is more feasible for minor vascular injuries, whereas interposition with an autologous venous graft is more appropriate for major injuries [4].
- In this case, endarterectomy and thrombectomy via arteriotomy for reversing ischemia were performed because the injured femoral artery was grossly free and soft tissue loss was relatively small. However, despite routine antibiotic prophylaxis and using appropriate antibiotics based on culture sensitivity, severe sepsis occurred. Furthermore, reinforcement and angioplasty for hemorrhage from the repaired artery failed.
- In the setting of sepsis, a prosthetic vascular graft is not commonly chosen. For patients requiring a bypass, an autologous graft is more favorable because a prosthetic graft is more susceptible to infection and thrombosis, particularly in patients with sepsis or at high risk of infection [4,5]. In addition, in cases of prosthetic infection after surgery for arterial disease, reconstruction with an autologous vein provides good potential for salvaging limbs and life [6]. Despite the risks above, in our case, a prosthetic graft was used in the setting of femoral sepsis with significant soft tissue loss because the saphenous vein had an insufficient length and diameter for graft reconstruction.
- Some alternative methods exist for this condition, such as a sartorius muscle rotation flap on femoral vessels, a rifampin-soaked graft, or a cryopreserved human allograft [7–9]. Certain studies have reported that the use of a bioactive heparin-treated expanded PTFE graft could provide more favorable outcomes, with a reduced incidence of the above-mentioned complications such as thrombosis and amputation, making it a potential alternative if an autologous saphenous vein is unavailable [10]. Vascular reconstruction by extraanatomic bypass with a ringed PTFE graft is also favorable for patients with vascular graft infection manifesting in the groin [11]. In this situation, as with inguinal-area infections, obturator bypass would be preferred [12]. Madden et al. [13] showed that lateral femoral bypass can be an alternative approach.
- Extraanatomic bypass with a prosthetic vascular graft is technically challenging in the setting of sepsis, but revascularization with a synthetic graft through an extraanatomic route can be successful. Of course, an autologous vein is more favorable for bypass to avoid thrombosis and uncontrolled infection. However, if an autologous vein is unsuitable because of the patient’s medical condition or the length of the vein, interpositioning an extraanatomic graft that avoids the infected surgical site can be considered early.
DISCUSSION
-
Ethical statements
This study was approved by the Institutional Review Board of Dankook University Hospital (No. DKUH 2022-06-29). The requirement for informed consent was waived by the Institutional Review Board.
-
Conflicts of interest
The authors have no conflicts of interest to declare.
-
Funding
None.
-
Author contributions
Project administration: SWC; Visualization: DSM; Writing–original draft: SWC; Writing–review & editing: all authors.
All authors read and approved the final manuscript.
ARTICLE INFORMATION


- 1. Siddique MK, Bhatti AM. A two-year experience of treating vascular trauma in the extremities in a military hospital. J Pak Med Assoc 2013;63:327–30. PubMed
- 2. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 2013;41:580–637. ArticlePubMed
- 3. Szilagyi DE, Smith RF, Elliott JP, Vrandecic MP. Infection in arterial reconstruction with synthetic grafts. Ann Surg 1972;176:321–33. ArticlePubMedPMC
- 4. Akingba AG, Robinson EA, Jester AL, et al. Management of vascular trauma from dog bites. J Vasc Surg 2013;58:1346–52. ArticlePubMed
- 5. Bell CL, Ali AT, Brawley JG, et al. Arterial reconstruction of infected femoral artery pseudoaneurysms using superficial femoral-popliteal vein. J Am Coll Surg 2005;200:831–6. ArticlePubMed
- 6. Nevelsteen A, Lacroix H, Suy R. Autogenous reconstruction with the lower extremity deep veins: an alternative treatment of prosthetic infection after reconstructive surgery for aortoiliac disease. J Vasc Surg 1995;22:129–34. ArticlePubMed
- 7. Landry GJ, Carlson JR, Liem TK, Mitchell EL, Edwards JM, Moneta GL. The sartorius muscle flap: an important adjunct for complicated femoral wounds involving vascular grafts. Am J Surg 2009;197:655–9. ArticlePubMed
- 8. Oderich GS, Bower TC, Hofer J, et al. In situ rifampin-soaked grafts with omental coverage and antibiotic suppression are durable with low reinfection rates in patients with aortic graft enteric erosion or fistula. J Vasc Surg 2011;53:99–106. ArticlePubMed
- 9. Bossi M, Tozzi M, Franchin M, et al. Cryopreserved human allografts for the reconstruction of aortic and peripheral prosthetic graft infection. Ann Vasc Dis 2017;10:391–7. ArticlePubMedPMC
- 10. Dorigo W, Di Carlo F, Troisi N, et al. Lower limb revascularization with a new bioactive prosthetic graft: early and late results. Ann Vasc Surg 2008;22:79–87. ArticlePubMed
- 11. Meyer T, Schweiger H, Lang W. Extraanatomic bypass in the treatment of prosthetic vascular graft infection manifesting in the groin. Vasa 1999;28:283–8. ArticlePubMed
- 12. Patel A, Taylor SM, Langan EM 3rd, et al. Obturator bypass: a classic approach for the treatment of contemporary groin infection. Am Surg 2002;68:653–8. ArticlePubMedPDF
- 13. Madden NJ, Calligaro KD, Dougherty MJ, Zheng H, Troutman DA. Lateral femoral bypass for prosthetic arterial graft infections in the groin. J Vasc Surg 2019;69:1129–36. ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite



