Articles
- Page Path
- HOME > J Trauma Inj > Volume 34(2); 2021 > Article
-
Original Article
Comparative Evaluation of Emergency Medical Service Trauma Patient Transportation Patterns Before and After Level 1 Regional Trauma Center Establishment: A Retrospective Single-Center Study - Hyeong Seok Lee, M.D.1, Won Young Sung, M.D.1,2, Jang Young Lee, M.D.1,2, Won Suk Lee, M.D.1,2, Sang Won Seo, M.D.1
-
Journal of Trauma and Injury 2021;34(2):87-97.
DOI: https://doi.org/10.20408/jti.2020.0021
Published online: March 24, 2021
- 3,165 Views
- 128 Download
- 2 Crossref
1Department of Emergency Medicine, Daejeon Eulji Medical Center, Daejeon, Korea
2Department of Emergency Medicine, Eulji Universitiy, School of Medicine, Daejeon, Korea
- Correspondence to Won Young Sung, M.D. Department of Emergency Medicine, Daejeon Eulji Medical Center, 95 Dunsanseo-ro, Seo-gu, Daejeon 35233, Korea Tel: +82-42-611-3256 Fax: +82-42-611-3880 E-mail: sage77@hanmail.net
Copyright © 2021 The Korean Society of Traumatology
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Purpose
- This study examined emergency medical service (EMS) transportation patterns for adult trauma patients before and after establishing a level 1 regional trauma center (RTC) and to evaluate the transportation approach after prehospital severity screening.
-
Methods
- This was a retrospective observational study of trauma patients aged ≥18 years admitted via EMS to the emergency department or a level 1 RTC, 1 year before to 3 years after RTC establishment. Patients with an Injury Severity Score (ISS) in the patient registration system were selected. Analyses were performed to determine transportation pattern changes by comparing patients pre- and post-RTC establishment and by yearly comparisons over the 4-year study period using the Mann-Whitney U test and chi-square test.
-
Results
- Overall, 3,587 patients were included. The mean ISS was higher in the post-RTC group (n=2,693; 10.63±8.90, median 9.00) than in the pre-RTC group (n=894; 9.44±8.20, median 8.00; p<0.001). The mean transportation distance (9.84±13.71, median 5.80 vs. 13.12±16.15 km, median 6.00; p<0.001) was longer in the post-RTC group than in the pre-RTC group. Furthermore, proportionally fewer patients were transported from an area in the same city as the RTC after establishment (86.1% vs. 78.3%; p<0.001). Yearly comparisons revealed a gradually increasing trend in the hospital death rate (ptrend=0.031).
-
Conclusions
- After establishing a level 1 RTC, the EMS transportation of severe trauma patients increased gradually along with the long-distance transportation of minor trauma patients. Therefore, improved prehospital EMS trauma severity assessments and level 1 RTC involvement in patient classification in the prehospital phase are necessary.
- Trauma, the eighth main cause of death worldwide, is also a major cause of death in the Republic of Korea [1]. Particularly, in young people (10 to 30 years of age), intentional self-harm (suicide) and road traffic accidents are the top two causes of death [2]. Trauma causes socioeconomic losses owing to serious sequelae and delayed return to daily life [3]. The 2009–2010 rate of preventable trauma fatalities in the Republic of Korea was 29.8%, a level higher than those of other developed countries (10–20%), and this discrepancy spurred the establishment of level 1 regional trauma centers (RTCs) in Korea [4]. In 2012, in support of level 1 RTCs, a project was initiated to establish such centers equipped with appropriate facilities, equipment, and manpower. This project aimed at providing severe trauma patients with optimal treatment (including emergency surgery) within 24 hours after hospital arrival, 365 days per year. By evenly distributing Korea’s RTCs such that treatment can commence for trauma patients within an hour of arrival, it was expected that the preventable trauma fatality rate could be reduced to <20% [3].
- By 2020, 15 level 1 RTCs were being operated in Korea. Governmental efforts have focused on establishing a standard operating system for RTCs by reviewing RTC operation criteria, as well as by conducting operational-level examinations. Since level 1 RTCs are established to provide intensive treatment to a unique group of severe trauma patients, the scope and type of services should differ from those of emergency departments (EDs).
- Severe trauma patients, who comprise the primary patient group treated at level 1 RTCs, are transported via emergency medical services (EMS; in Korea EMS include 119 emergency medical technicians, who provide primary care at the prehospital stage and during transportation to the hospital). To provide optimal treatment, RTCs need to be organically and independently operated. However, EMS personnel must understand that level 1 RTCs should provide specialized treatment to trauma patients only, unlike the broader range of services provided in the ED. A misunderstanding also exists that a regional trauma system can be operated simply by establishing trauma centers. Due to these misconceptions, the number of minor trauma patients at level 1 RTCs has continued to increase [5].
- Thus, to prevent problems from arising, EMS must actively transport severe trauma patients to level 1 RTCs and distribute the transportation of uncomplicated minor trauma patients. Furthermore, it is necessary to compare EMS transportation before and after level 1 RTC establishment. However, no previous study anywhere in the world has compared EMS trauma patient transportation before and after level 1 RTC establishment. Accordingly, this study aimed to compare the EMS transportation patterns of trauma patients (including adult trauma patients with injuries of various severity transported by EMS, patient transportation time and distance, and the area the patient was transported from) before and after level 1 RTC establishment.
INTRODUCTION
- Study design and setting
- The regional trauma center where the study was conducted is located in the center of a metropolitan city with a population of about 1.47 million and an area of about 68 km2. There are 26 EMS centers in the city and 962 paramedics are active. The city has two regional emergency medical centers, four local emergency medical centers, and five local emergency medical facilities. The hospital that conducted the study consists of an RTC and a local emergency medical center, and all trauma patients visiting the center are treated by the RTC medical staff. The center does not operate helicopter services.
- This retrospective study was conducted on trauma patients aged ≥18 years transported via EMS and admitted to the ED before RTCs were established (the ED provided support before the establishment of level 1 RTCs through the governmental project) or at the level 1 RTC after it was established. The study was approved by the Institutional Review Board of the Daejeon Eulji Medical Center (IRB No. 2019-07-001), and the requirement for informed consent was waived.
- Selected trauma patients were identified using the hospital trauma registration system as having come to the ED (via EMS within 1 year before establishment of the level 1 RTC), or to the RTC (via EMS within 3 years after establishment), and had an Injury Severity Score (ISS) in the registration system. Exclusion criteria were as follows: those transferred by helicopter, those transferred from another hospital to the ED or to a level 1 RTC after initial EMS transportation to that hospital first; those who died immediately after arriving at the ED or the RTC (rendering it impossible to estimate the ISS), and those for whom information was missing from the prehospital care reports (on transportation time, transportation distance, or on the area the patient was transported from).
- Data collection and classification
- Data on age, sex, the mechanism of trauma, and death were collected from patients’ medical charts. The ISS was obtained from data collected and organized by the trauma coordinators at the trauma center. The ISS was not measured for patients discharged after treatment at the ED or RTC. Information on transportation time and distance, as well as the area the patient was transported from, was obtained by reviewing prehospital care reports. When patients were transferred from the metropolitan city where the center is located, they were classified as coming from “downtown”, while other areas were classified as “out of town”.
- The mechanism of trauma, specified in the medical charts, was categorized into one of the following 10 groups based on the Korea Triage and Acuity Scale: traffic accident involving four-wheeled motor transportation (passenger car, van, jeep, truck, and bus); traffic accident involving two-wheeled motor transportation (including motorcycle); traffic accident involving non-motorized transportation (including bicycle); other traffic accidents; falls; slip down; blunt injury; penetrating injury; injury caused by a machine; other types of trauma; and trauma of unknown cause. The area where the patient was transported from was classified as in or outside the city of the RTC location. Transportation time was estimated in minutes based on the interval between EMS contact time with the patient and arrival time at the RTC. Transportation distance was measured in driving distance in kilometers, between the reporting address received by the EMS and the RTC. ISS <15 or ≥15 points were classified as minor and severe trauma, respectively.
- Data analysis
- In this article, continuous variables are presented as means±standard deviations with median values, and categorical variables as percentages (%). Two approaches were used to classify patients into groups for the analysis. The first approach compared patients before and after the establishment of the level 1 RTC. In this approach, the pre-RTC group consisted of patients admitted to the ED 1 year before RTC establishment, while those in the RTC group were admitted to the RTC within 3 years of its establishment. Continuous and categorical data were compared using the t-test and chi-square analysis, respectively. For continuous variables that were not normally distributed, the Mann-Whitney U test was used for comparison.
- The goal of the second approach was to compare the 1-year period before RTC establishment with three 1-year intervals post-RTC establishment. Thus, four groups were formed. Group A included patients who were admitted to the ED within 1 year before RTC establishment while groups B, C, and D included those who were admitted to the RTC in years 1, 2, and 3, respectively, after its establishment. Between-group differences in age, ISS, and transportation time and distance were examined using one-way analysis of variance, while between-group differences in sex, number of hospital deaths, area where the patients were transported from, and the number of minor and severe trauma patients were examined using the chisquare test. Trends were analyzed using the Cochran-Armitage trend test.
- For all analyses, 95% confidence intervals were calculated, and differences were considered to be statistically significant if the p-value was <0.05. Data analysis was performed using SPSS version 24 (IBM Corp., Armonk, NY, USA) and R software version 3.6.0 (R Project for Statistical Computing., Vienna, Austria).
METHODS
- Study population
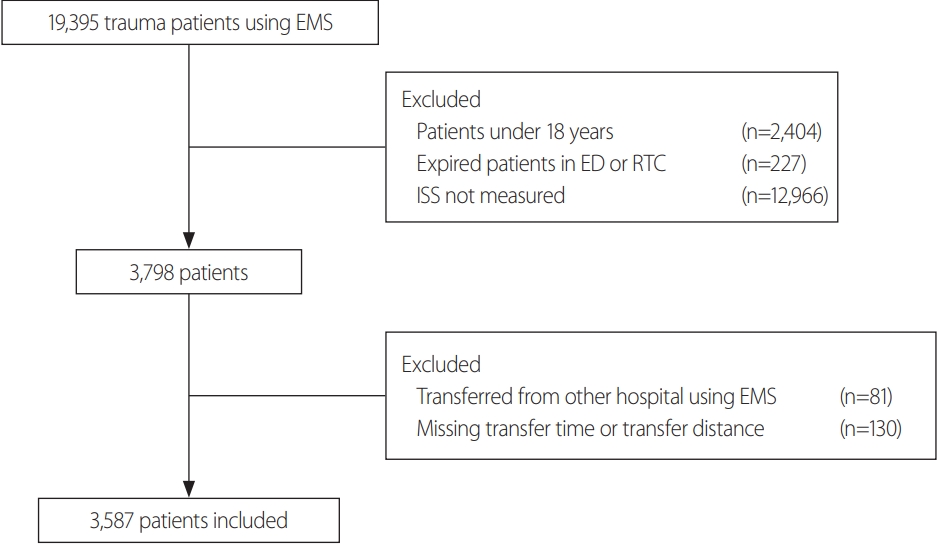
- Over the 4-year study period, of the 19,395 trauma patients admitted, 2,404 patients were <18 years old and 227 died either in the resuscitation room of the ED or the RTC. A total of 12,966 patients with no ISS scores were excluded. Of the 3,798 patients with ISS, 81 who were transferred from another hospital and 130 with missing information (on transportation time and distance) were also excluded. Finally, 3,587 patients were included as the study subjects (Fig. 1). The total number of patients and excluded patients according to the criteria for each group (A, B, C and D) are shown in Table 1.
RESULTS
- General comparison
- Of the 3,587 patients, 894 and 2,693 were in the preRTC and RTC groups, respectively. The patients in the RTC group had a higher mean age (53.68±19.00 years, median 53.00 years vs. 55.80±19.12 years, median 57.00 years; p=0.004); mean ISS (9.44±8.20, median 8.00 vs. 10.63±8.90, median 9.00; p<0.001); mean transportation time (22.24±14.25 minutes, median 19.00 vs. 24.19±16.22 minutes, median 20.00 minutes; p=0.001); and mean transportation distance (9.84±13.71 km, median 5.80 km vs. 13.12±16.15 km, median 6.00 km; p<0.001) than those in the pre-RTC group. The proportion of men was higher than that of women in both groups (57.6% vs. 61.5%; p=0.038). Other characteristics are shown in Table 2.
- Comparison of characteristics by RTC and ISS groups
- Significantly different proportions of minor (ISS <15) and severe (ISS ≥15) trauma patients were observed in the pre-RTC and RTC groups, with a higher proportion of severe trauma patients in the RTC group (18.8% vs. 23.2%; p=0.006) (Table 3).
- Among the minor trauma patients, the RTC group had higher mean ISS (6.16±3.69, median 5.00 vs. 6.59±3.41, median 5.00; p=0.010) and transportation distance (9.55±12.26 km, median 5.45 km vs. 12.49±15.90 km, median 6.00 km; p<0.001) than the pre-RTC group, while the hospital death rate was lower in the RTC group (p=0.005) (Table 3). In the severe trauma patient group, the RTC group had a higher hospital death rate (p=0.044) and mean transportation distance (9.08±10.89 km, median 6.00 km vs. 15.04±17.88 km, median 7.00 km; p<0.001; however, no significant between-group differences were found in the mean ISS (23.62±7.17, median 22.00 vs. 24.01±8.33, median 22.00; p=0.921) and mean transportation time (20.79±12.89 minutes, median 18.00 minutes vs. 24.65±17.38 minutes, median 19.00 minutes; p=0.069) (Table 3).
- Comparison by accident district
- Pre- and post-RTC comparisons were made based on the area from which patients were transported (downtown or out of town). For the downtown group, mean age (53.49±19.23 years, median 53.00 years vs. 55.22±19.47 years, median 56 years; p=0.024) and mean ISS (9.44±8.24, median 8.00 vs. 10.21±8.74, median 9.00; p=0.035) were higher in the RTC group; however, in the RTC group, the mean transportation time was lower (18.67±8.16 minutes, median 17.00 vs. 18.02±8.30 minutes, median 16.00 minutes; p=0.022). The hospital death rate (p=0.813) and the mean transportation distance (5.78±4.39 km, median 5.00 km vs. 6.21±5.13 km, median 5.00 km; p=0.113) did not differ significantly between groups (Table 4).
- For those transported from out of town, the RTC group showed a higher mean ISS (9.46±8.01, median 8.00 vs. 12.13±9.29, median 9.00; p<0.001), higher hospital death rate (p=0.016), and higher mean transportation distance (35.05±22.35 km, median 30.00 km vs. 38.09±17.67 km, median 34.00 km; p=0.006). However, mean age (54.91±17.48 years, median 55.00 years vs. 57.91±17.65 years, median 59.00 years; p=0.085) and mean transportation time (44.40±21.99 minutes, median 41.00 vs. 46.48±18.17 minutes, median 43.00 minutes; p=0.064) did not differ significantly between groups (Table 4).
- Comparison of characteristics by RTC group, ISS, and accident district
- The proportion of downtown patients (transported from an area in the same city as the RTC) with severe trauma (ISS ≥15) was similar in the pre-RTC and RTC groups (18.6% vs. 21.6%; p=0.078). Further, none of the characteristics (ISS, hospital death rate, transportation time, and distance) showed significant between-group differences (p>0.05 for all). In the downtown patients with minor trauma (ISS <15), the hospital death rate was significantly lower in the RTC group (4.5% vs. 2.2%; p=0.004). No other characteristic was significantly different between the groups (p>0.05) (Table 5).
- Among the out-of-town patients, the proportion of severe trauma patients did not differ between the pre-RTC and RTC groups (20.2% vs. 28.9%; p=0.060). However, in out-of-town patients with severe trauma (ISS ≥15), the RTC group showed a significantly higher hospital death rate (4.0% vs. 25.4%; p=0.017), a significantly longer mean transportation time (38.60±17.07 minutes, median 35.00 vs. 45.00±19.88 minutes, median 40.00 minutes; p=0.043), and a significantly longer mean transportation distance (29.44±13.44 km, median 25.00 km vs. 39.80±18.74 km, median 35.00 km; p=0.002) than the pre-RTC group. For minor trauma patients, the RTC had a significantly higher mean ISS (6.10±3.78, median 5.00 vs. 7.29±3.68, median 9.00; p=0.004), but no significant between-group differences were found for any other characteristics (Table 5).
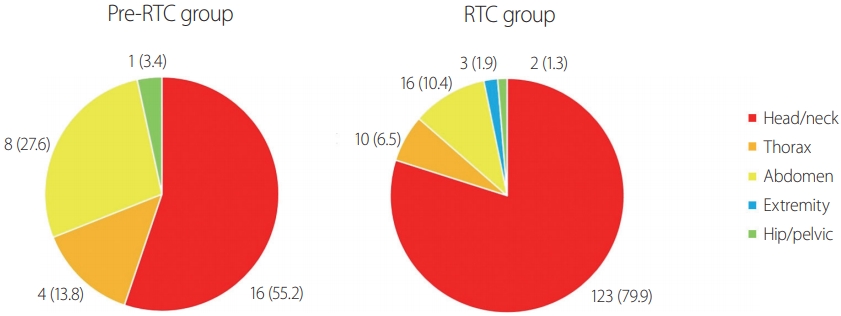
- Comparison of causes of death in hospitals by location of the injury
- An analysis of cause of death in hospitals by the location of the injury showed a significant difference between the pre-RTC and RTC groups in head and neck injuries (55.2% vs. 79.9%; p=0.025); followed by injuries in the abdomen (27.6% vs. 10.4%) and chest (13.8% vs. 6.5%) (Fig. 2).
- Yearly comparisons pre- and post-level 1 RTC establishment
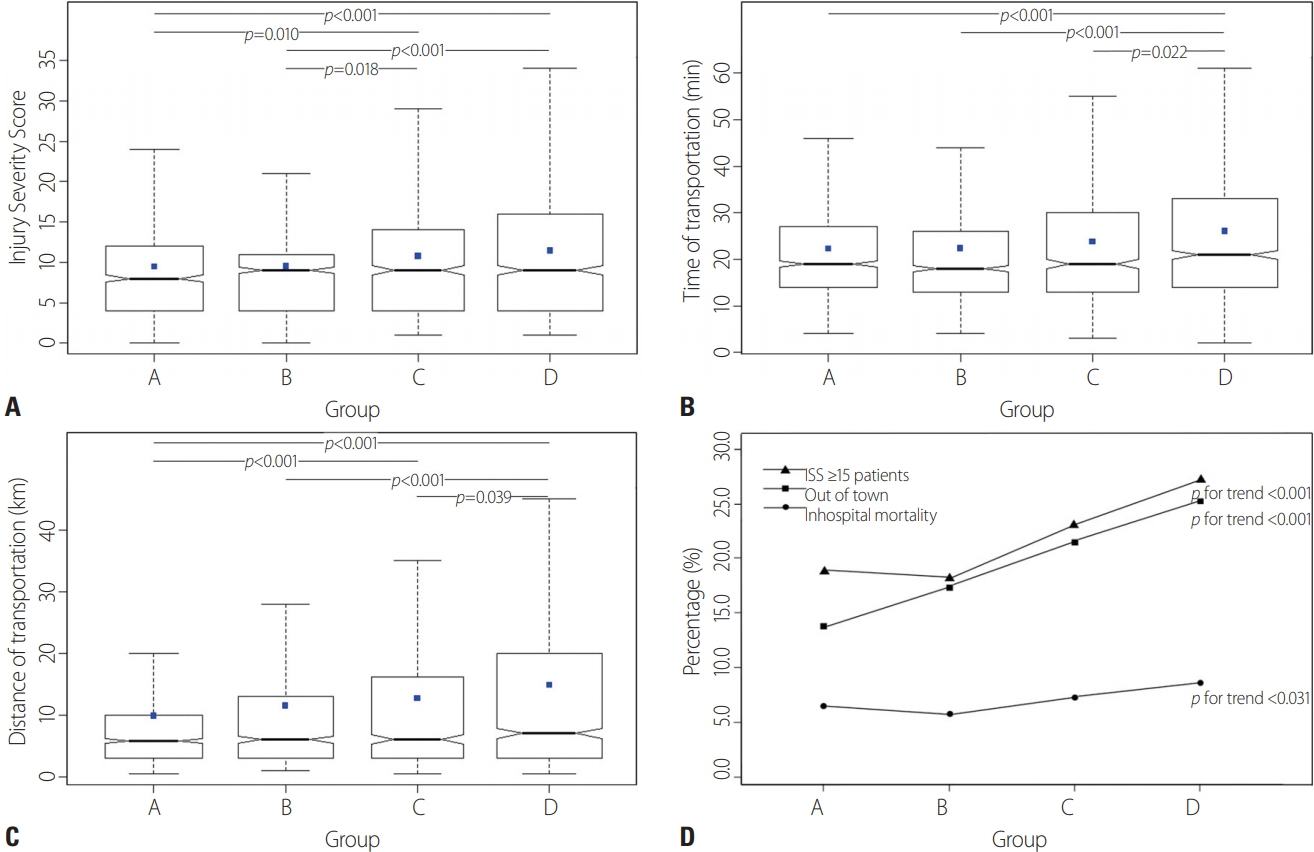
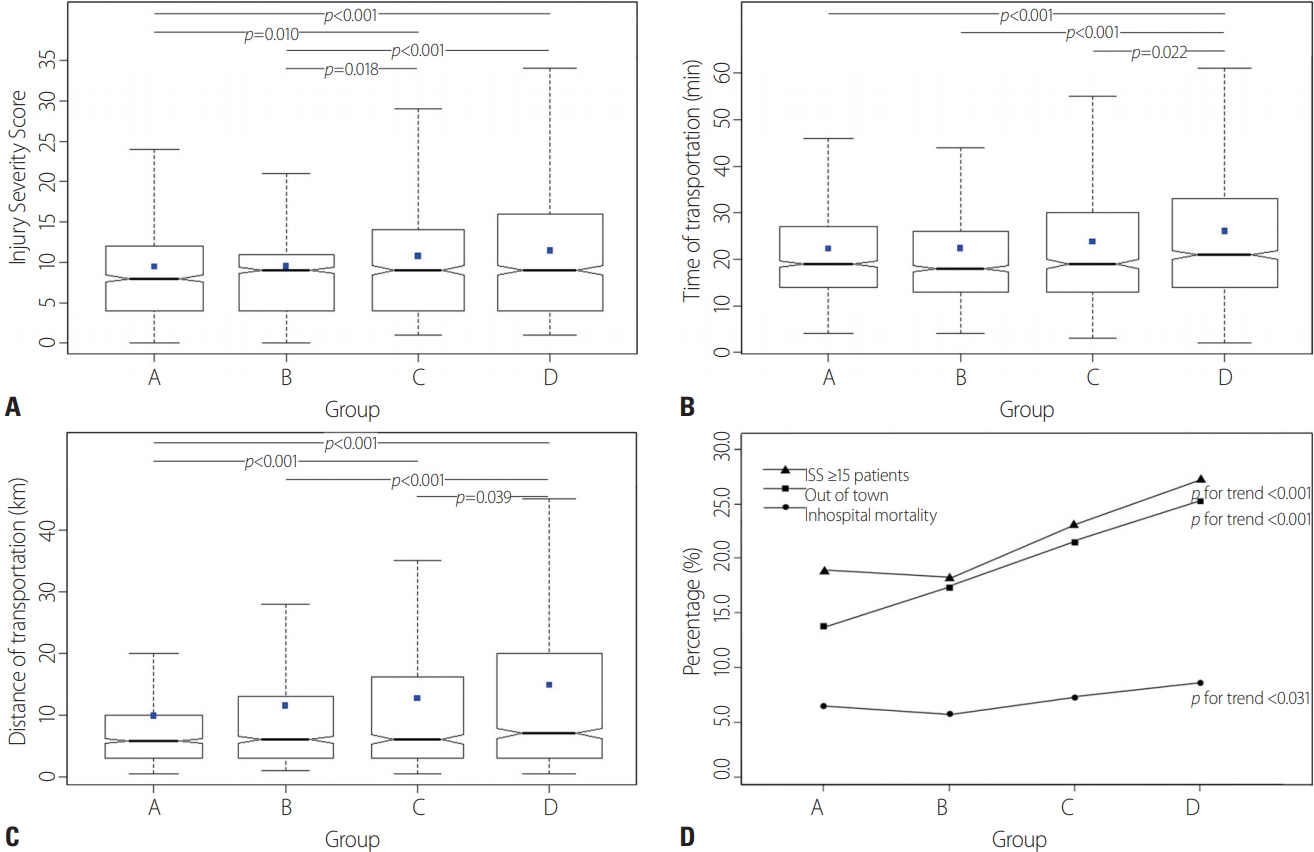
- The 1-year data before RTC establishment (group A) and data for the 3 years after establishment (groups B, C, and D) were compared yearly. The mean ISS was 9.44±8.20, 9.50±7.98, 10.76±9.56, and 11.44±8.98 in groups A, B, C, and D, respectively. Significant differences were observed between groups A and C (p=0.010), A and D (p<0.001), B and C (p=0.018), and B and D (p<0.001). An increasing trend occurred in the hospital death rate, which was 6.6%, 5.8%, 7.3%, and 8.7% in groups A, B, C, and D, respectively (p=0.031) (Fig. 3).
- In the four groups, the mean transportation time was 22.24±14.25, 22.36±14.48, 23.75±15.85, and 26.02±17.60 minutes, respectively, with significant differences between groups A and D (p<0.001), B and D (p<0.001), and C and D (p=0.022). The mean transportation distance was 9.84±13.71, 11.47±14.96, 12.71±15.33, and 14.78±17.51 km, respectively, with significant differences between groups A and C (p<0.001), A and D (p<0.001), B and D (p<0.001), and C and D (p=0.039) (Fig. 3).
- The proportion of patients transported from out of town was 13.9%, 17.4%, 21.5%, and 25.3% in groups A, B, C, and D, respectively, with a gradually increasing trend over time (p<0.001) (Fig. 3). The proportion of severe (ISS ≥15) trauma patients was 18.8%, 18.2%, 23.1%, and 27.3% in groups A, B, C, and D, respectively, with a gradually increasing trend over time (p<0.001) (Fig. 3).
Comparisons before and after RTC establishment
- An examination of minor and severe trauma patients classified using the ISS-based criterion showed that the proportion of minor trauma patients decreased, while that of severe trauma patients increased after the trauma center was established. The hospital death rate increased in severe trauma patients after the establishment of the trauma center, but the mean ISS of severe trauma patients did not differ between pre- and post-establishment.
- The mean transportation distance was higher after the trauma center opened than before it was established. The separate analyses of transportation distance for minor and severe trauma patients also showed the same pattern, with an increased transportation distance after the trauma center opened. According to the yearly comparisons from 1 year before the trauma center opened to 3 years after, the mean ISS and the proportion of severe trauma patients increased in the 3 post-opening years compared with 1 year before the opening. Further, mean transportation distance and time increased in the 3 post-opening years for both minor and severe trauma patients, similar to the findings of the analyses conducted to compare the pre- and post-opening findings of all trauma patients.
- In the analysis by accident district, in trauma patients initially transported from an area in the same city as the trauma center, the proportions of minor and severe trauma patients, as well as mean transportation distance and time, were similar pre- and post-opening of the trauma center. In patients transported from an area outside of the city, the mean ISS and mean transportation distance showed a significant difference pre- and post-opening. For severe trauma patients transported from an area outside of the city, the mean transportation time and distance increased after the trauma center opened.
- The study findings demonstrate positive changes after the establishment of the level 1 RTC. That is, EMS transported increasingly more severe trauma patients or patients suspected of having severe trauma to the RTC. However, given the finding that the mean transportation time and distance in minor trauma patients also increased, it seems that minor trauma patients still continued to be transported over long distances to the trauma center. The hospital mortality rate is thought to have increased after RTC establishment because there was a much higher proportion of patients with head and neck injuries after the trauma center opened than previously, and fatalities were higher for patients with head and neck injuries than for those with other injury types [6].
- The prehospital patient assessment currently used in Korea is based on the “Guidelines for EMS Emergency Response”, first established in 2011 [7]. As specified in the prehospital care report, the level of consciousness, pupillary reflex, and vital signs are evaluated; and in severe trauma cases, an assessment is performed in accordance with the detailed severe trauma assessment table. These guidelines are based on the Guidelines for Field Triage of Injured Patients proposed in the US in 2011. According to these guidelines, the hospital to which trauma patients are transported is determined on the basis of the trauma severity, assessed based on physiological criteria, anatomical area, the mechanism of injury, and other factors determined at the discretion of EMS [7,8].
- In a study conducted before the establishment of level 1 RTCs, Kim et al. [9] compared trauma severity assessments performed at the hospital to those performed by EMS in the field and found that only the vital signs assessment showed medium-level agreement, while the physical examination and the assessment of the mechanism of injury did not show high agreement. Hence, it is not easy to determine the level of hospital to which trauma patients should be transported based on severity assessments conducted only using the current guidelines for EMS emergency response. Further, it is impossible to use ISS at the prehospital phase to determine which patients should be transported to level 1 RTCs, because the ISS is derived after several tests are performed and a diagnosis has been made at the hospital. Recently, Lee et al. [10] reported that a prehospital evaluation of patient severity by measuring the Glasgow Coma Scale (GCS) and Revised Trauma Score (RTS) was helpful in assessing the severity of trauma patients. To assess trauma severity, it is necessary to evaluate the validity and utility of GCS or RTS, and the assessment items should be revised to follow, in a more multifaceted manner, the current guidelines for EMS emergency response and guidance in the prehospital care report.
- Lastly, it is necessary to ensure that severe trauma patients who require treatment that can be provided only by level 1 RTCs are appropriately transported by continuing to improve the EMS guidelines for patients’ transportation, as well as the table of detailed severe trauma assessment items in the prehospital care report. To do so, the EMS data on patient transportation (including detailed trauma case records) gathered so far should be made completely public so that additional research can be conducted and EMS quality control can be strengthened. It is thought that through this process, disagreements between EMS and level 1 RTCs with respect to trauma patient transportation will be resolved.
- In addition, improvements can be made by continuing to train EMS personnel, establishing a trauma system consisting of level 1 RTCs and local autonomous governments, and forming consortiums to organically link EMS within the region. At some university hospital trauma centers in the United States, trauma center nurses responsible for patient classification play the role of a central control center for EMS in their immediate communities. They participate in activating the trauma team at the hospital by providing consultation on the classification and transportation of ED patients and monitoring patient transportation in real time [5]. In Korea, level 1 RTCs should be involved more proactively in prehospital patient classification and patient transportation through direct communication between trauma center medical staff and EMS.
- This study has a few limitations. First, the study analyzed trauma patients admitted to a single level 1 RTC. Due to regional limitations, the study sample may not be representative of level 1 RTCs nationwide; therefore, the findings should be interpreted with caution. In the future, multicenter studies should be conducted to examine data at the national level. Second, trauma patients aged <18 years were excluded from the study. It is not common for the ISS to be calculated in children, and the score that distinguishes between severe and minor trauma patients when using the ISS differs from that used for assessing adults [11]. Third, the methodology used a retrospective study design. Because the study was based on the review and analysis of medical charts and prehospital care reports, possible errors owing to incorrect recordings and missing information could not be avoided. Finally, because the scope of information that can be obtained from prehospital care reports is limited, factors such as the traffic situation impacting patient transportation time and distance or the situation of other hospitals were not considered in analysis. Additionally, the data entered into the table of detailed severe trauma assessment items and other detailed data on severe trauma patients transported to the level 1 RTC were not available to the authors; therefore, it was impossible to confirm whether or not EMS transported patients in accordance with the guidelines for EMS emergency response. In the future, these data should be disclosed so that research can be conducted on EMS prehospital trauma patients’ transportation to level 1 RTCs.
- No previous study has yet compared EMS trauma patients before and after RTC establishment. This study confirmed changes in EMS transportation patterns before and after the establishment of the trauma center for. In the future, a nationwide survey of patients transported to RTCs by EMS is needed. A pre-hospital evaluation study of EMS is also needed, with the detailed evaluation of severe trauma.
DISCUSSION
- Although EMS transportation of severe trauma patients to the level 1 RTC increased after the trauma center opened, long-distance transportation of minor trauma patients persisted after the establishment of a level 1 RTC. To address this problem, EMS should improve the methods used for prehospital trauma severity assessment, and level 1 RTCs should also be involved in the prehospital phase for severity assessment and patient transportation in the region.
CONCLUSION

| Group Aa | Group Bb | Group Cc | Group Dd | Total | |
|---|---|---|---|---|---|
| Total patients | 4,558 | 4,647 | 4,499 | 5,691 | 19,395 |
| Patients under 18 years | 626 | 608 | 605 | 565 | 2,404 |
| Expired patients in ED or RTC | 56 | 61 | 54 | 56 | 227 |
| ISS not measured | 2,920 | 3,070 | 2,999 | 3,977 | 12,966 |
| Transferred from other hospital using EMS | 18 | 22 | 16 | 25 | 81 |
| Missing transfer time or transfer distance | 44 | 40 | 21 | 25 | 130 |
| Number of patients included | 894 | 846 | 804 | 1,043 | 3,587 |
ED: emergency department, RTC: regional trauma center, ISS: Injury Severity Score, EMS: emergency medical service.
a Patients who were admitted to the ED within 1 year of RTC establishment.
b Patients who were admitted to the RTC in year 1.
c Patients who were admitted to the RTC in year 2.
d Patients who were admitted to the RTC in year 3.
- 1. World Health Organization (WHO). Disease burden and mortality estimates [Internet]. Geneva:: WHO; 2018 [cited 2020 Mar 1]. Available from: https://www.who.int/healthinfo/global_burden_disease/estimates/en/.
- 2. Statics Korea. 2018 causes of death statistics [Internet]. Daejeon: Statics Korea; 2019 [cited 2020 Mar 1]. Available from: http://kostat.go.kr/portal/korea/kor_nw/1/6/2/index.board?bmode=read&bSeq=&aSeq=377606&pageNo=1&rowNum=10&navCount=10&currPg=&searchInfo=&sTarget=title&sTxt.
- 3. Park JM. Outcomes of the support services for the establishment of regional level 1 trauma centers. J Korean Med Assoc 2016;59:923–30. Article
- 4. Kim H, Jung KY, Kim SP, Kim SH, Noh H, Jang HY, et al. Changes in preventable death rates and traumatic care systems in Korea. J Korean Soc Emerg Med 2012;23:189–97.
- 5. Ministry of Health and Welfare. Establishment of a standard operating system for regional trauma centers [Internet]. Sejong: Ministry of Health and Welfare; 2019 [cited 2020 Mar 1]. Available from: https://www.prism.go.kr/homepage/entire/retrieveEntireDetail.do?pageIndex=1&research_id=1351000-201900020&leftMenuLevel=160&cond_research_name=%EA%B6%8C%EC%97%AD%EC%99%B8%EC%83%81%EC%84%BC%ED%84%B0&cond_research_start_date=&pageUnit=10&cond_order=3.
- 6. Curtis KA, Mitchell RJ, Chong SS, Balogh ZJ, Reed DJ, Clark PT, et al. Injury trends and mortality in adult patients with major trauma in New South Wales. Med J Aust 2012;197:233–7. ArticlePubMed
- 7. National Fire Agency. The standard protocols for 119 emergency medical services providers [Internet]. Sejong: National Fire Agency; 2019 [cited 2020 Mar 1]. Available from: http://www.nfa.go.kr/nfa/publicrelations/legalinformation/0017/0003/?boardId=bbs_0000000000001097&-mode=view&cntId=4&category=&pageIdx=&searchCondition=&searchKeyword=.
- 8. Sasser SM, Hunt RC, Faul M, Sugerman D, Pearson WS, Dulski T, et al. Guidelines for field triage of injured patients: recommendations of the National Expert Panel on Field Triage, 2011. MMWR Recomm Rep 2012;61:1–20.
- 9. Kim DK, Hong KJ, Noh H, Hong WP, Kim YJ, Shin SD, et al. Measure of agreement between prehospital EMS personnel and hospital staffs using guidelines for field triage of injured patients. J Trauma Inj 2014;27:126–32.
- 10. Lee SY, Cheon YJ, Han C. Comparison prehospital RTS (revised trauma score) with hospital RTS in trauma severity assessment. J Trauma Inj 2015;28:177–81. ArticlePDF
- 11. Brown JB, Gestring ML, Leeper CM, Sperry JL, Peitzman AB, Billiar TR, et al. The value of the Injury Severity Score in pediatric trauma: Time for a new definition of severe injury. J Trauma Acute Care Surg 2017;82:995–1001. ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
- Establishment of Emergency Teaching Model and Optimization of Discrete Dynamic Calculation in Complex Virtual Simulation Environment
He Li, Yuansong Sun, Kai Song, Chunlin Yin, Gengxin Sun
Mathematical Problems in Engineering.2022; 2022: 1. CrossRef - Model for Predicting In-Hospital Mortality of Physical Trauma Patients Using Artificial Intelligence Techniques: Nationwide Population-Based Study in Korea
Seungseok Lee, Wu Seong Kang, Sanghyun Seo, Do Wan Kim, Hoon Ko, Joongsuck Kim, Seonghwa Lee, Jinseok Lee
Journal of Medical Internet Research.2022; 24(12): e43757. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite