Comparison of Resting Energy Expenditure Using Indirect Calorimetry and Predictive Equations in Trauma Patients: A Pilot Study
Article information
Abstract
Purpose
Nutritional therapy in the intensive care unit is an essential factor for patient progress. The purpose of this study was to compare resting energy expenditure (REE) calculated by prediction equations (PEs) to the REE measured by indirect calorimetry (IC) in trauma patients.
Methods
Patients admitted to the trauma intensive care unit who received mechanical ventilation between January and December 2015 were enrolled. REE was measured by IC (CCM Express, MGC Diagnostics) and calculated by the following PEs: Harris-Benedict, Fleisch, Robertson and Reid, Ireton-Jones, and the maximum value (25 kcal/kg/ day) of the European Society for Clinical Nutrition and Metabolism (ESPEN). All patients were ventilated at a fraction of inspired oxygen (FiO2) below 60%.
Results
Of the 31 patients included in this study, 24 (77.4%) were men and seven (22.6%) were women. The mean age of the patients was 49.7±13.2 years, their mean weight was 68.1±9.6 kg, and their mean Injury Severity Score was 26.1±11.3. The mean respiratory quotient on IC was 0.93±0.19, and their mean FiO2 was 38.72%±6.97%. The mean REE measured by IC was 2,146±444.36 kcal/day, and the mean REE values calculated by the PEs were 1,509.39±205.34 kcal/day by the Harris and Benedict equation, 1,509.39±154.33 kcal/day by the Fleisch equation, and 1,443.39±159.61 kcal/day by the Robertson and Reid equation. The Ireton-Jones equation yielded a higher value (2,278.90±202.35 kcal/ day), which was not significantly different from the value measured using IC (p=0.53). The ESPEN maximum value (1,704.03±449.36 kcal/day) was lower, but this difference was likewise not significant (p=0.127).
Conclusions
The REE measured by IC was somewhat higher than that calculated using PEs. Further studies are needed to determine the proper nutritional support for trauma patients.
INTRODUCTION
Nutritional therapy for critically ill patients is an essential factor for patient progress. Especially in trauma patients, changes in energy metabolism, such as hypermetabolism, result in undernutrition or overnutrition if proper nutritional support is not supplied [1]. Undernutrition has been found to be related to poor wound healing, an increased risk of infections, impaired muscle function, and reduced cardiac and respiratory reserve [2]. Overnutrition, in contrast, may induce respiratory compromise, cause hepatic dysfunction, and increase the risk of infection [3-5].
Currently, indirect calorimetry (IC) is the accepted gold standard for measuring resting energy expenditure (REE) [6]. Several studies have shown that IC is more accurate than predictive equations (PEs) in determining the energy needs of critically ill patients, including traumatized patients [5,7,8]. However, measuring REE by IC is not always available, as it requires expensive equipment and trained personnel. Thus, many critical care physicians still rely on various PEs to estimate the caloric needs of patients. These PEs, such as the Harries-Benedict, Fleisch, Robertson and Reid, Ireton-Jones, and the maximum value (25 kcal/kg/day) of the European Society for Clinical Nutrition and Metabolism (ESPEN) equations, have been established and validated for estimating REE in various clinical states [9-13].
In the current study, we compared the REE measured by IC with that calculated using the five abovementioned PEs. We sought to determine which of these equations better reflected the REE measured by IC in patients with severe trauma.
METHODS
This was a retrospective, observational, and analytical study. All patients were admitted to the trauma intensive care unit (ICU) at Gachon University Gil Medical Center from January to December 2015. This study was approved by the Research Ethics Committee of Research and Education. The need for informed consent was waived because additional procedures were not performed except for routine intensive care, and the data collection did not exceed the normal risk of harm to the participant. This study was approved by the Institutional Review Board of the Gil Medical Center of Gachon University College of Medicine (IRB No. GCIRB2017-389). Informed consent was waived by The Ethics Committee of Gil Medical Center of Gachon University College of Medicine. Our work does not infringe on the rights of others, including privacy rights and intellectual property rights. There were no human rights violations in our study.
Mechanically ventilated patients in whom REE was measured by IC were enrolled. This study was designed to include patients aged >18 years with an Injury Severity Score (ISS) of >15. The fraction of inspired oxygen (FiO2) was 0.6 or less while measuring REE with IC. Patients with a FiO2 >0.6 on the ventilator settings or a respiratory quotient (RQ) outside of the physiological range were excluded. IC was performed using a CCM Express® indirect calorimeter (MGC Diagnostics, St. Paul, MN, USA). The calorimeter was operated during the study period by two dedicated members of our nutritional support team, who had expertise in the technique. The patients were sedated and maintained at -2 on the Richmond agitation–sedation scale (RASS) during the evaluation. The REE measurement by IC was performed 15 minutes after reaching a steady state of -2 on the RASS.
Demographic data of the patients were obtained at the time of ICU admission. Body mass index (BMI) was calculated using the following formula: BMI=weight (kg)/height squared (m2). Body surface area (BSA) was calculated using the Du Bois formula [14]: BSA (m2)=0.007184×weight0.425 (kg)×height0.725 (cm). The REE was estimated using five predictive methods: the Harris and Benedict, Fleisch, Robertson and Reid, and Ireton-Jones equations, and the ESPEN maximum value (Table 1).

Five predictive equations for calculating REE in this study
Statistical analyses were performed using SPSS version 19.0 (IBM Corp., Armonk, NY, USA). Data were reported as means±standard deviations (SD) or as medians and interquartile ranges, as appropriate. The paired t-test was used to evaluate the differences between the measured REE and that calculated by PEs. The Bland-Altman method was used to calculate the mean difference in REE measured by IC with that calculated using PEs. For each PE, accuracy was defined as an estimated value within ±10% of the measured REE for an individual. Statistical significance was set at p<0.05.
RESULTS
The demographic data are shown in Table 2. A total of 31 patients (male/female: 24/7) were included in this study. All patients were aged >18 years, with a mean age of 49.7±13.2 years. Their mean BMI was 24.7±3.1 kg/m2, and their mean BSA was 1.77±0.15 m2. The mean duration of ventilator use was 10.2±6.0 days, and the mean duration of the ICU stay was 16.8±13.8 days. Among the 31 patients, 26 (83.9%) had blunt injuries and five (16.1%) had penetrating injuries (stab wounds). The mean ISS was 26.1±11.3. The ISS was >15 in all patients. The mean time lag from trauma until measurement of the IC was 3.6±1.9 days, and most patients had IC measurements made within 7 days. The ventilator status of all patients was stable within an FiO2 of 60%, with a mean of 38.72±6.97%. The mean RQ was 0.93±0.19. On ICU admission, 61.2% of the patients underwent an emergency operation, 25.8% underwent laparotomy, and 12.9% underwent thoracotomy. Table 3 shows a comparison of the measured and predicted REE values. The mean REE measured by IC was 2,146±444.36 kcal/day, and the mean REE calculated by the PEs was 1,509.39±205.34 kcal/day for the Harris and Benedict question, 1,509.39±154.33 kcal/day for the Fleisch equation, and 1,443.39±159.61 kcal/day for the Robertson and Reid equation. These three PEs yielded estimated REEs that were significantly lower than the REE measured by IC (p=0.006, p=0.003, and p<0.001, respectively). The Ireton-Jones equation yielded a higher value (2,278.90±202.35 kcal/day) than the measured REE, but the difference was not significant (p=0.053). The ESPEN maximum value (1,704.03±449.36 kcal) was lower, but the difference was not significant (p=0.127). Fig. 1 shows the measured and calculated REE of each individual. Fig. 2 shows the Spearman's correlation coefficients and a scatter plot graph between the IC and each PE. All PEs revealed a positive correlation with IC (0.264≤r≤0.521). The Ireton-Jones equation showed the highest correlation with IC (r=0.521), while ESPEN had the lowest correlation (r=0.264).
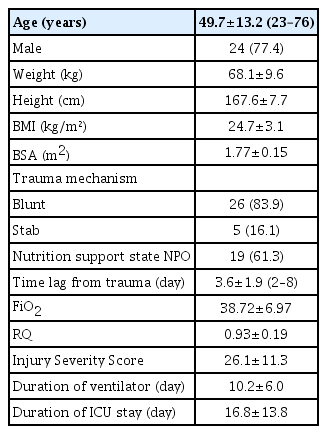
Demographic data of patients (n=31)

Comparison of REE between indirect calorimetry and predictive equations
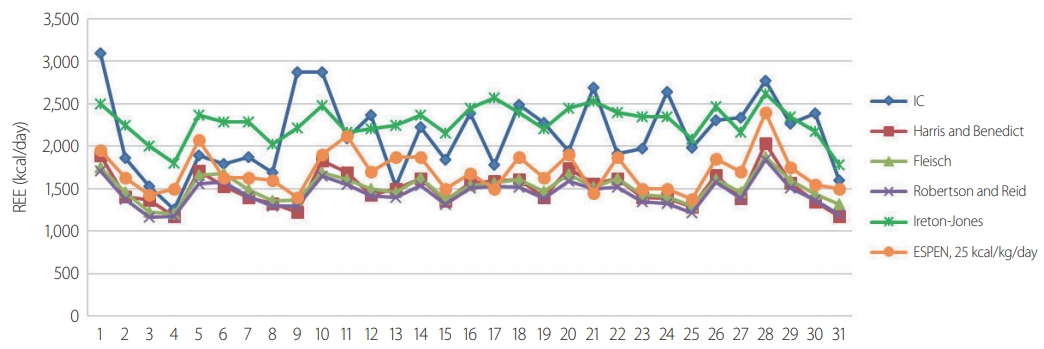
The measured and calculated REE of individuals. REE: resting energy expenditure, IC: indirect calorimetry, ESPEN: European Society for Clinical Nutrition and Metabolism.

Spearman's correlation coefficients and scatter plot graph between the IC and each PE. IC: indirect calorimetry, ESPEN: European Society for Clinical Nutrition and Metabolism, PE: prediction equation.
In terms of the agreement of the PEs with IC at the individual level, the Harris-Benedict, Fleisch, and Robertson-Reid equations revealed similar results in this study (Harris-Benedict, 9.6% agreement and 90.4% underestimation; Fleisch, 9.5% and 90.4%; and Robertson and Reid, 6.5% and 93.4%, respectively). The ESPEN maximum value (25 kcal/kg) agreed with IC in 25.8% of cases and was an underestimation in 74.2% of cases. Unlike the other equations, the Ireton-Jones equation showed agreement in 41.9% of cases, overestimation in 45.1%, and underestimation in 12.9%. Fig. 3 shows the Bland-Altman plot for REE between the five PEs and IC. All five predictive equations showed fixed bias in the Bland-Altman plot.
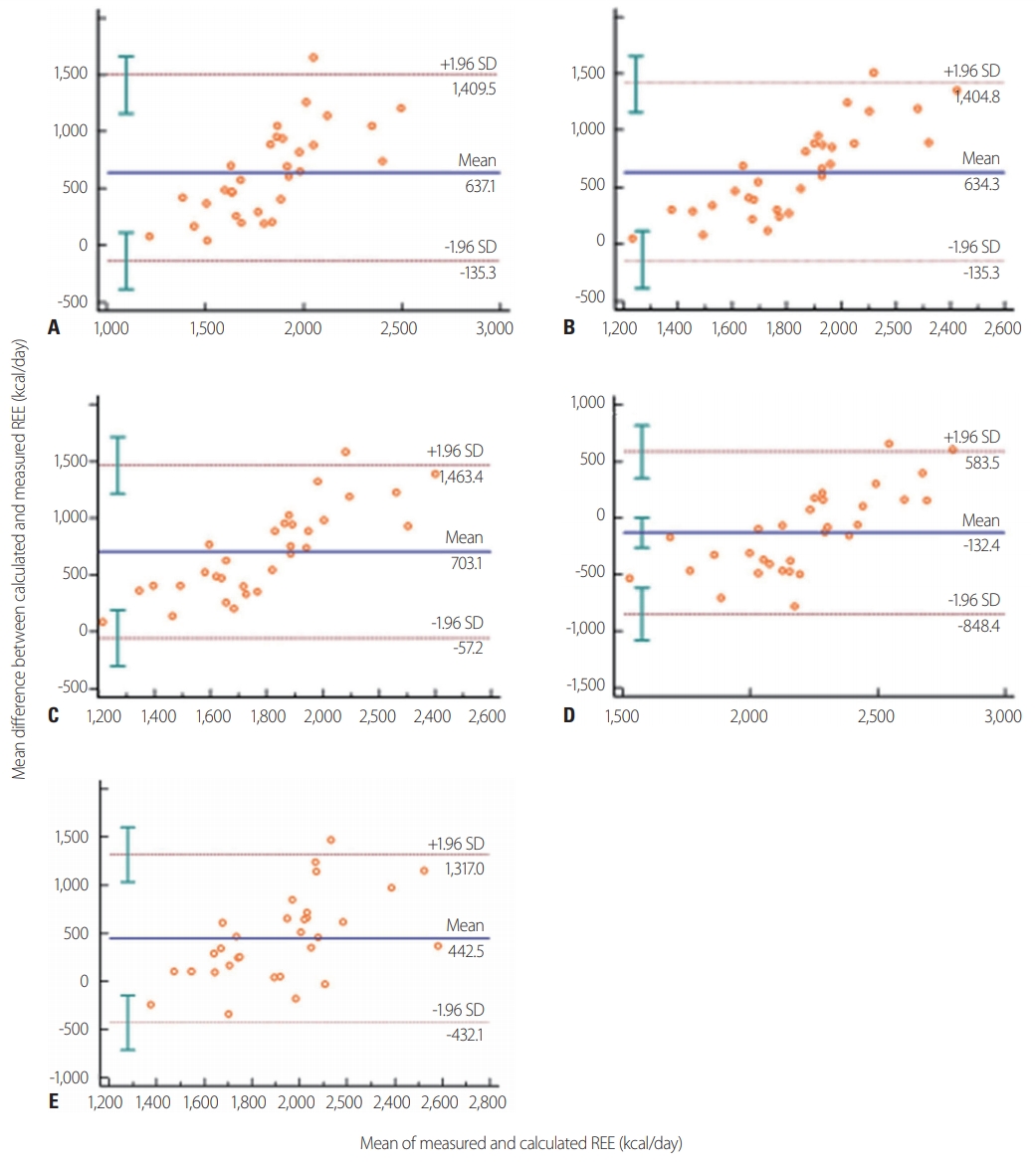
Bland-Altman plots comparing predictive equations and measured energy expenditure by indirect calorimetry: (A) Harris-Benedict method; (B) the Fleisch equation; (C) the Robertson and Reid equation; (D) the Ireton-Jones equation; (E) the ESPEN maximum value (25 kcal/kg). The middle dashed horizontal line represents the absolute bias (mean difference between the two methods in kcal/day). The upper and lower dashed lines depict the 95% limits of agreement (mean difference±1.96 SD). REE, resting energy expenditure, SD: standard deviations, ESPEN: European Society for Clinical Nutrition and Metabolism.
DISCUSSION
Nutritional support must be based on an accurate assessment of the patient’s energy expenditure (EE) to avoid complications associated with inadequate nutritional support [1-5]. An individual’s EE is generally assessed by estimating the REE, which accounts for approximately 70% of the total EE. The REE can be estimated by using PEs or IC [6]. The calculated REE based on PEs could have limitations in fully responding to physiological and metabolic variability with regard to its application in practical nutrition. Various environmental conditions and physiological factors affect EE [15]. Measuring REE using IC, which quantifies oxygen consumption and carbon dioxide production, provides a more accurate approximation of EE [5,7,8,16]. Several studies have compared IC with PEs in various medical conditions [17-19].
Despite the standardization of REE measurements by IC in various clinical situations, few studies have compared the REE as assessed by PEs and IC, specifically in severe trauma patients with mechanical ventilation. In 1996, Monk et al. [20] evaluated sequential changes in the metabolic response after blunt trauma, including 10 patients on a ventilator. Among their results, it was reported that measured REE was significantly higher than predicted REE, averaging 55% above the predicted value. In 2000, Plank and Hill [1] also reported similar results in 12 patients with severe trauma, where REE was measured by IC as the ratio to the predicted REE; they found that the ratio increased over the first 4 to 5 days and peaked around days 9 to 12, with a peak ratio of 1.60±0.13 during trauma. The above-mentioned studies showed similar results for patients with severe trauma, as the measured REEs were higher than the calculated REEs for a certain period after trauma.
Although the accuracy and reliability of REE using IC have been accepted, its use is limited in clinical settings because of personnel qualifications, logistics, and economic issues [16]. Thus, calculating the REE using PEs is still an available method.
In this study, we evaluated the accuracy of five commonly used PEs against measured REE in 31 patients with severe trauma (ISS >15) on ventilators in the ICU. The correlation between each PE and the REE measurement was positive and significant (r≥0.372, p≤0.040), with the exception of the ESPEN maximum value (r=0.264, p=0.152). The Ireton-Jones equation was the PE with the highest accuracy in comparison with the IC values (41.9%). In a comparison of the mean REE values using the paired t-test, as shown in Table 2, the estimated REE using PEs presented relatively lower values except for the Ireton-Jones equation. Our data showed that all of the equations, except the Ireton-Jones equation, underestimated REE in severe trauma patients.
There are some limitations to this study. First, this was a retrospective study with a small sample. Second, we were unable to simultaneously obtain body weight while measuring REE with IC. This may have influenced the difference in the final REE values obtained using PEs in this study. Third, each subject was measured once; therefore, it was not possible to estimate intra-individual variation in REE. Fourth, although all participants in this study were trauma patients, we could not identify the impact of specific injury patterns on energy requirements individually. Sixth, this study did not assess clinical outcomes according to the REE.
CONCLUSION
The REE measured by IC was relatively higher than the REE calculated by PEs, except for the REE calculated using the Ireton-Jones equation. We recommend using IC when assessing caloric requirements after trauma, as in our study group. Further development of more practical methods that can accurately predict energy needs is desirable.