Articles
- Page Path
- HOME > J Trauma Inj > Volume 30(4); 2017 > Article
-
Case Report
Hepatic Hemangioma Rupture Caused by Blunt Trauma - Gil Hwan Kim, M.D.1, Jae Hun Kim, M.D.1, Sang Bong Lee, M.D.2
-
Journal of Trauma and Injury 2017;30(4):235-237.
DOI: https://doi.org/10.20408/jti.2017.30.4.235
Published online: December 30, 2017
- 5,261 Views
- 47 Download
- 1 Crossref
1Department of Trauma Surgery, Pusan National University Hospital, Busan, Korea
2Department of Surgery, Pusan National University Yangsan Hospital, Yangsan, Korea
- Correspondence to: Jae Hun Kim, M.D., Department of Trauma Surgery, Pusan National University Hospital, 179 Gudeok-ro, Seo-gu, Busan 49241, Korea, Tel: +82-51-240-7369, Fax: +82-51-240-7719, E-mail: jjangmdkmdk@hanmail.net
• Received: November 7, 2017 • Revised: December 14, 2017 • Accepted: December 14, 2017
Copyright © 2017 The Korean Society of Trauma
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Hepatic hemangioma is the most frequently occurring benign tumor of the liver. Hepatic hemangioma rupture is a rare phenomenon, which can lead to life-threatening conditions. Here, we report a case of hepatic hemangioma rupture caused by blunt trauma. Explorative laparotomy was performed due to unstable vital signs and abdominal massive hemoperitoneum revealed on computed tomography. We detected arterial bleeding from a hepatic hemangioma and performed primary suture of the liver and postoperative angiographic embolization.
- The liver is the most commonly injured organ from blunt abdominal trauma [1]. Hepatic hemangiomas are the most frequently occurring benign tumors of the liver. However, most patients are not aware of the existence of hemangiomas, which are incidentally diagnosed during imaging studies or surgical abdominal exploration [2]. Spontaneous or traumatic rupture of hepatic hemangioma is rare and can cause serious bleeding and life threatening conditions. We report a rare case of hepatic hemangioma rupture caused by blunt abdominal trauma.
INTRODUCTION
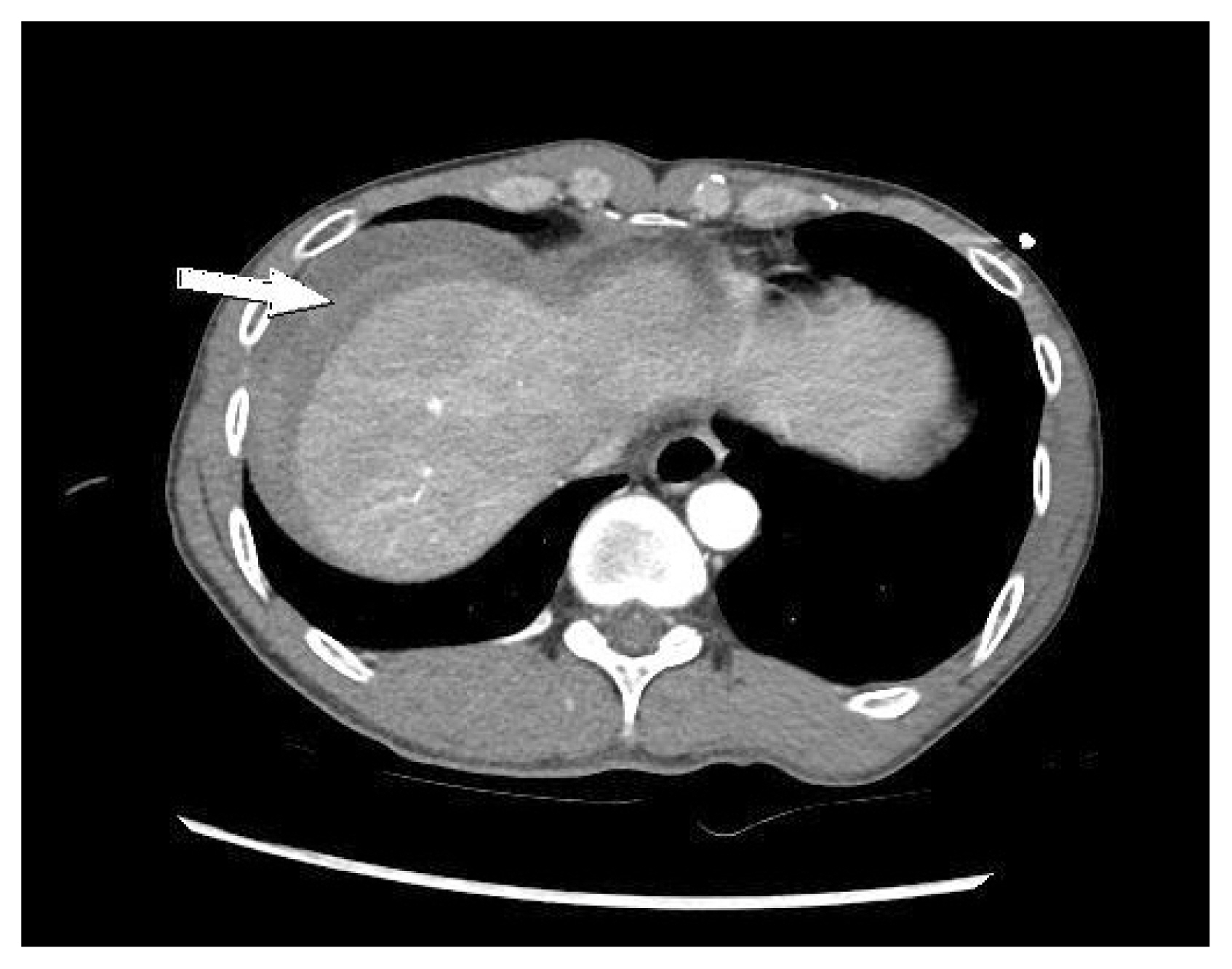
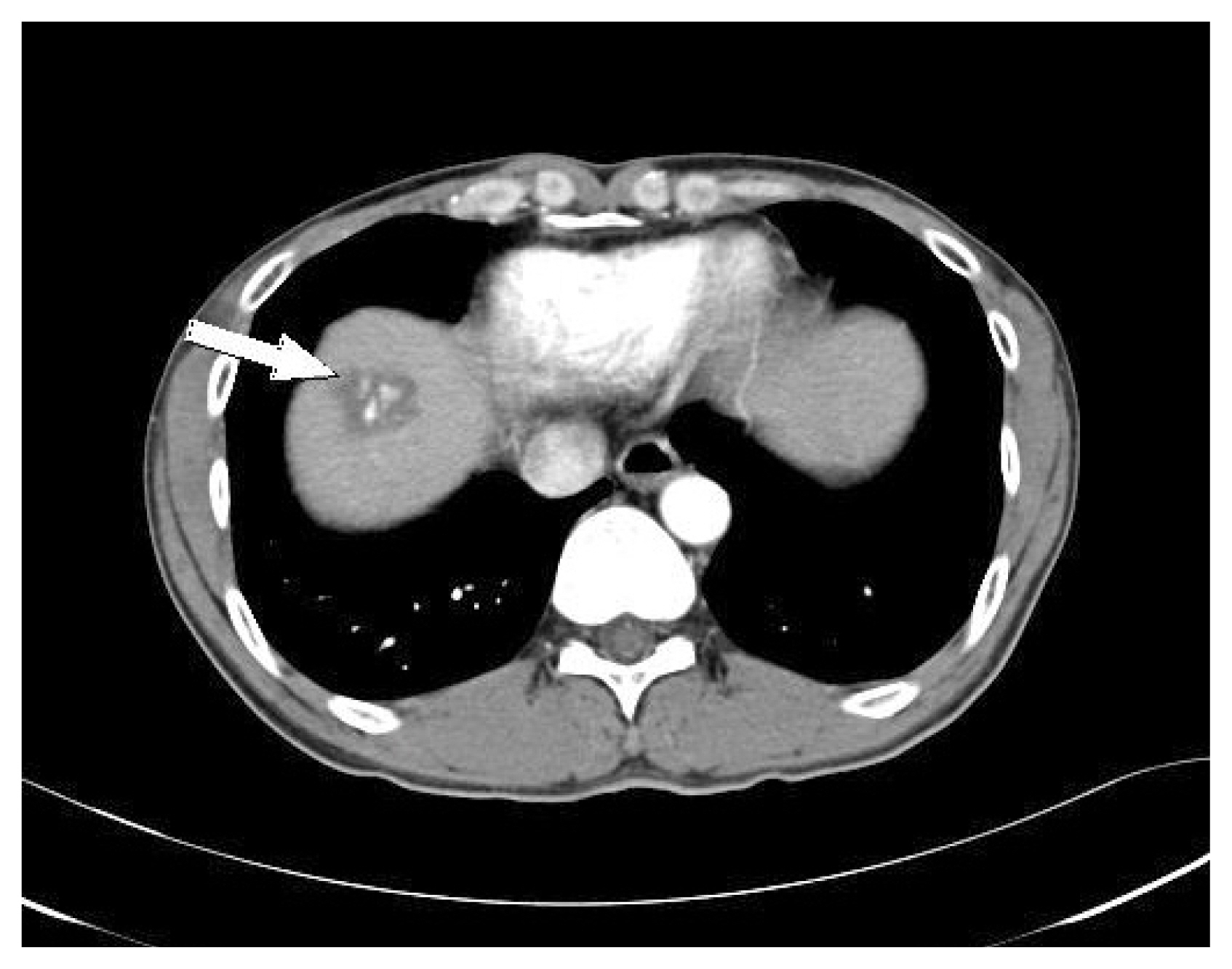
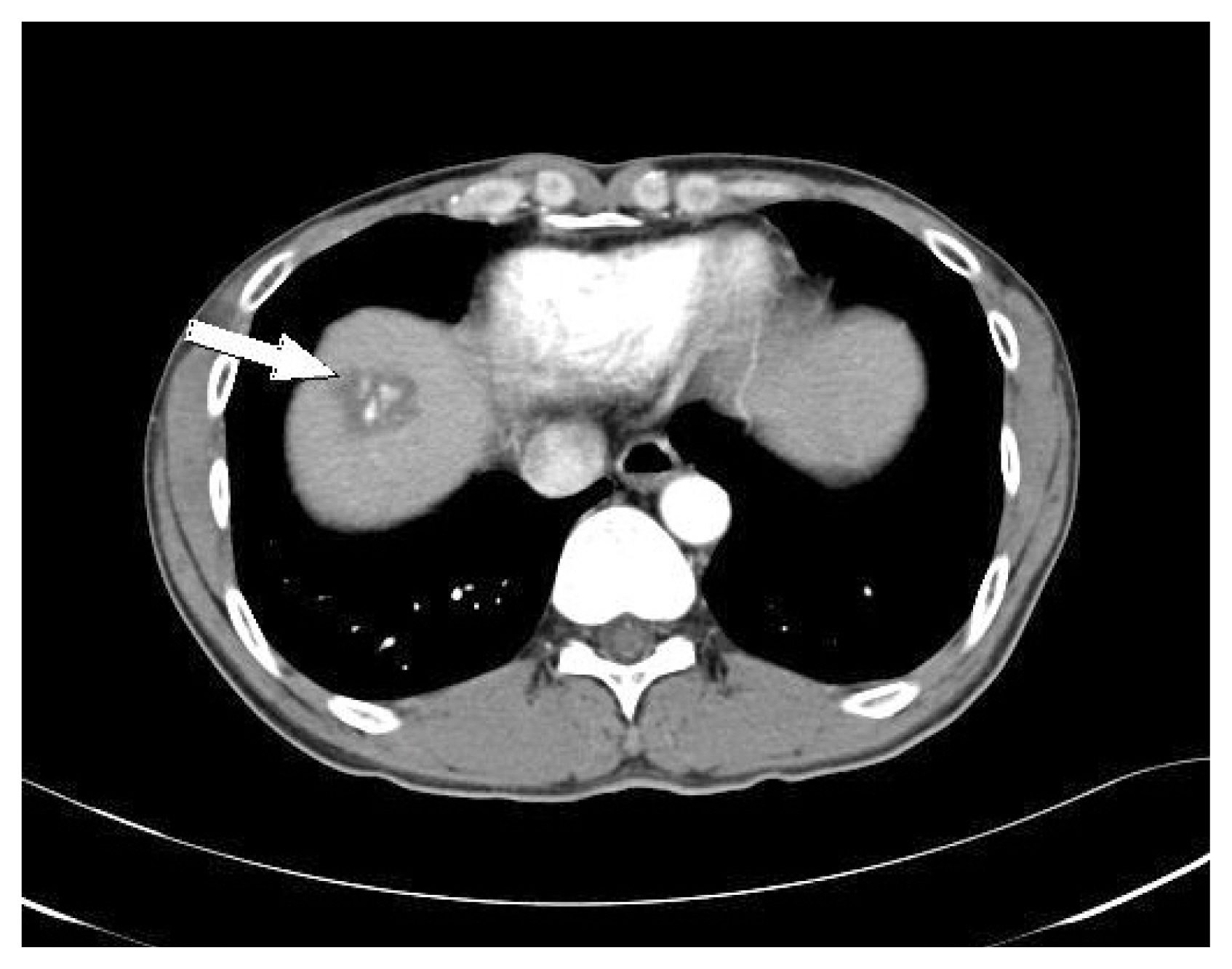
- A 46-year-old man with no prior medical history was transferred to our trauma center after falling from a height of 1 m. He was alert, and his vital signs were as follows: blood pressure was 80/50 mmHg, pulse rate was 96 beats/min, respiratory rate was 28 breaths/min, and body temperature was 36.6°C. Abdominal distension was noted, and focused assessment with sonography for trauma revealed fluid collection within Morrison’s pouch and splenorenal pouch. He had received blood transfusions at another hospital and initial hemoglobin was noted to be 11.9 g/dL at our trauma center. After resuscitation, abdominal computed tomography (CT) showed massive hemoperitoneum without a focus of active bleeding. We noted a 3.4 cm hepatic hemangioma in the liver dome (Fig. 1). Abdominal CT findings revealed, no focus of extravasation, but a sentinel clot sign was found in the perihepatic area (Fig. 2). We performed explorative laparotomy because of the large amount of hemoperitoneum and consistently low blood pressure. Surgical findings included more than 2 L blood and arterial bleeding from a hemangioma in the liver dome. We then performed primary suture of the surface of the hemangioma and immediate postoperative angiography. Angiography revealed hemangioma at liver dome with contrast blushes and embolization using gelatin sponge was performed. He was discharged without any complication 9 days postoperatively. The hemangioma had decreased in size 3 months later (Fig. 3).
CASE REPORT
- The prevalence of spontaneous rupture of hepatic hemangiomas ranges from 1% to 4%, and that of traumatic rupture remains unknown [2,3]. The mortality rate in patients with spontaneous or traumatic hepatic hemangioma rupture is approximately 35% [2].
- Most hepatic hemangiomas are asymptomatic, and they can cause right upper quadrant abdominal pain associated with necrosis or capsular distension as the tumor grows. When rupture occurs spontaneously or by trauma, symptoms such as sudden abdominal pain and distension with hemoperitoneum may appear, leading to coagulopathy and hypovolemic shock [2].
- Hepatic hemangiomas are usually incidentally diagnosed during imaging studies for another problem. Imaging studies used to diagnose hepatic hemangiomas include ultrasonography, dynamic contrast-enhanced CT, magnetic resonance imaging, and hepatic arteriography. On CT, hemangiomas show peripheral enhancement in the arterial phase. When hemangiomas rupture, radiologic findings show hemoperitoneum and a heterogeneous hepatic mass. As observed in the present case, intraperitoneal clots may also be identified near the site of the bleeding known as the sentinel clot sign [2].
- The treatment of unruptured hepatic hemangiomas is usually decided on the basis of the size and location of the tumor. Small asymptomatic hemangiomas can be conservatively managed; however, surgery is required for cases of ruptured hemangiomas with hemoperitoneum or coagulopathy. Although surgery may include resection or enucleation, damage control surgery, such as packing, hepatic artery ligation, or hepatic suture may be required in the case of ruptured hemangiomas with life-threatening conditions [4].
- Recently transcatheter arterial embolization (TAE) has been used in the treatment of hemangiomas, and for reducing the size of the tumor in cases of giant hemangiomas, or as a preoperative temporizing procedure in cases of ruptured hemangiomas. TAE as an alternative to surgical resection is controversial because of its complications, including postembolization pain, nausea, biliary tree damage, infection, liver abscess, and sepsis. However, owing to technical improvements and fewer complication rates, TAE has also been safely and effectively used as a single therapy in recent research [5–7]. If vital signs were stable, TAE without surgery would have been attempted in our case.
- Traumatic rupture of hepatic hemangioma is rare, but it can lead to life threatening conditions with massive bleeding. If a patient presenting with blunt trauma exhibits massive hemoperitoneum and a hepatic hemangioma is noted during history-taking or on an imaging study, the possibility of hemangioma rupture should be suspected. Although surgery may be required for treating a ruptured hepatic hemangioma, TAE can be a safe and effective treatment option if the vital signs are stable.
DISCUSSION
ACKNOWLEDGEMENTS
Fig. 1Initial computed tomography reveals massive hemoperitoneum and hepatic hemangioma in the liver dome with peripheral enhancement on the arterial phase (arrow).

Fig. 2The sentinel clot sign demonstrates a heterogeneous fluid collection (clot) that tends to accumulate near the site of the injury (arrow).
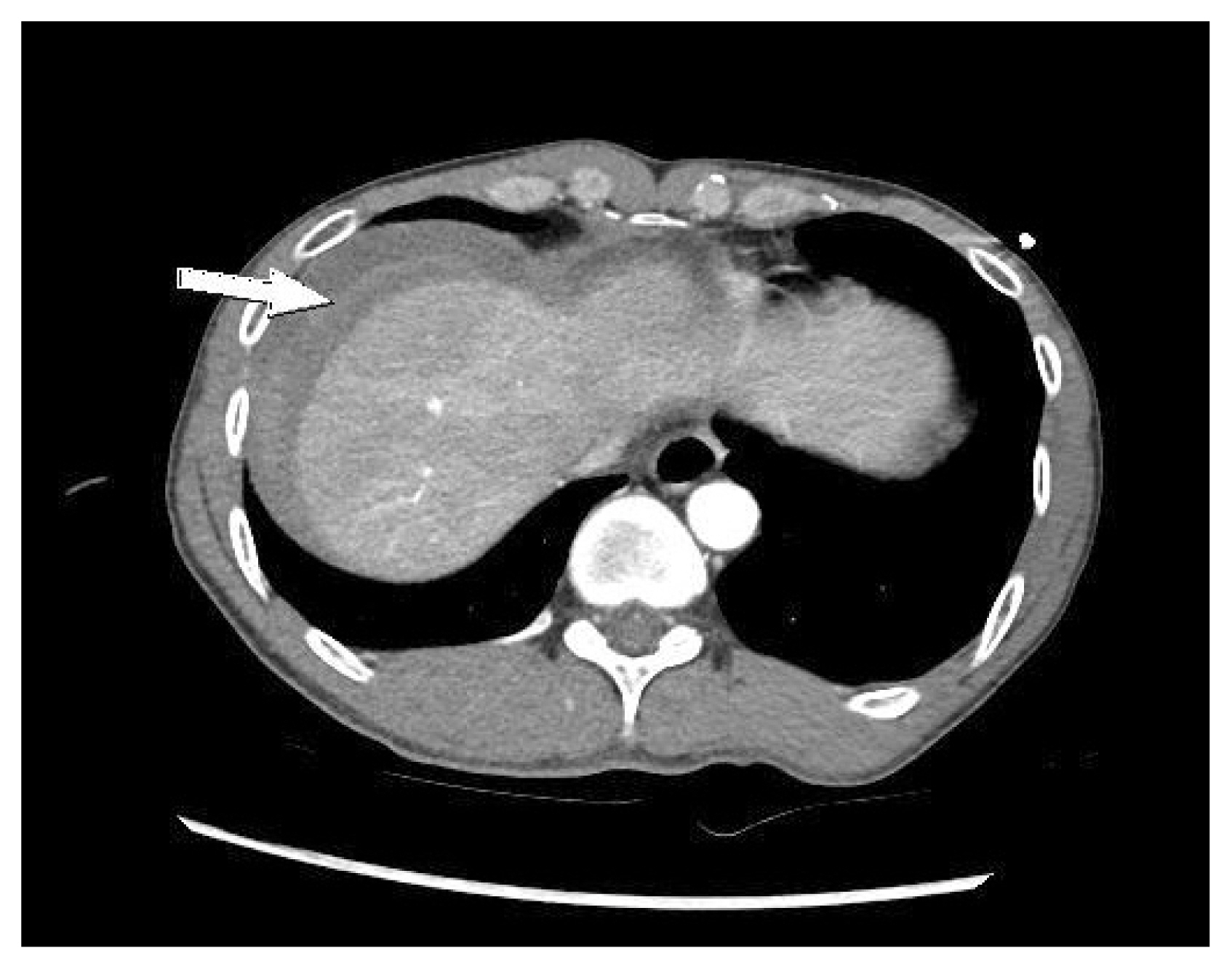
Fig. 3Computed tomography revealed slight decrease in the size of the hepatic hemangioma after three months (arrow).
- 1. Ahmed N, Vernick JJ. Management of liver trauma in adults. J Emerg Trauma Shock 2011;4:114–9.ArticlePubMedPMC
- 2. MA Jr, Papaiordanou F, Gonçalves JM, Chaib E. Spontaneous rupture of hepatic hemangiomas: a review of the literature. World J Hepatol 2010;2:428–33.ArticlePubMedPMC
- 3. Sung JE, Park SJ, Nam CW, Hwang JC, Kim YM. Traumatic rupture of a hepatic hemangioma. J Trauma Inj 2013;26:252–4.
- 4. Kang LY, Huang FD, Liu YY. Blunt abdominal injury with rupture of giant hepatic cavernous hemangioma and laceration of the spleen. Hepatobiliary Pancreat Dis Int 2015;14:109–10.ArticlePubMed
- 5. Mohan S, Gupta A, Verma A, Kathura MK, Baijal SS. Case report Non-surgical management of a giant liver hemangioma. Indian J Radiol Imaging 2007;17:81–3.Article
- 6. Giavroglou C, Economou H, Ioannidis I. Arterial embolization of giant hepatic hemangiomas. Cardiovasc Intervent Radiol 2003;26:92–6.ArticlePubMedPDF
- 7. Firouznia K, Ghanaati H, Alavian SM, Nassiri Toosi M, Ebrahimi Daryani N, Jalali AH, et al. Management of liver hemangioma using trans-catheter arterial embolization. Hepat Mon 2014;14:e25788, ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Post‐traumatic rupture of hepatic haemangioma
Tessa Gaynor, Vanshika Sinh, Jonathan Reddipogu
ANZ Journal of Surgery.2023; 93(11): 2754. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite