Articles
- Page Path
- HOME > J Trauma Inj > Volume 30(4); 2017 > Article
-
Case Report
Diagnostic Laparoscopy and Laparoscopic Diverting Sigmoid Loop Colostomy in Penetrating Extraperitoneal Rectal Injury: A Case Report - Young Goun Jo, M.D.1, Yun Chul Park, M.D.1, Wu Seong Kang, M.D.1, Jung Chul Kim, M.D.1, Chan Yong Park, M.D.2
-
Journal of Trauma and Injury 2017;30(4):216-219.
DOI: https://doi.org/10.20408/jti.2017.30.4.216
Published online: December 30, 2017
- 5,465 Views
- 26 Download
- 1 Crossref
1Division of Trauma Surgery, Department of Surgery, Chonnam National University Hospital, Gwangju, Korea
2Trauma Center, Pusan National University Hospital, Busan, Korea
- Correspondence to: Yun Chul Park, M.D., Division of Trauma Surgery, Department of Surgery, Chonnam National University Hospital, 42 Jebog-ro, Dong-gu, Gwangju 61469, Korea, Tel: +82-62-220-6456, Fax: +82-62-227-1635, E-mail: kontikithor@gmail.com
• Received: November 13, 2017 • Revised: December 8, 2017 • Accepted: December 9, 2017
Copyright © 2017 The Korean Society of Trauma
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
- Laparoscopy has been one of the most effective modalities in various surgical situations, although its use in trauma patients has some limitations. The benefits of laparoscopy include cost-effectiveness, shorter length of hospital stay, and less postoperative pain. This report describes diagnostic laparoscopy and laparoscopic diverting sigmoid loop colostomy in penetrating extraperitoneal rectal injury. A 41-year-old male presented with perineal pain following penetrating trauma caused by a tree limb. Computed tomography showed air density in the perirectal space and retroperitoneum. As his vital signs were stable, we performed diagnostic laparoscopy and confirmed no intraperitoneal perforation. Therefore, laparoscopic diverting sigmoid loop colostomy was performed. He was discharged without any complications despite underlying hepatitis C-related cirrhosis. Colostomy closure was performed 3 months later.
- Laparoscopy is commonly used for abdominal surgery and is a proven effective modality in an emergency setting [1]. However, many clinicians hesitate to use laparoscopy because of concern about missed injuries and bleeding control. Nonetheless, use of laparoscopy in trauma cases can reduce the morbidity associated with a negative laparotomy, and can be a reliable, minimally-invasive option for management of selected injuries in hemodynamically stable patients [2]. The management of an extraperitoneal rectal injury is dictated by its location. If the injury is distal and can be accessed by a transanal approach, repair should be performed [3]. However, some extraperitoneal injuries are difficult to repair because the injury site is too high for transanal repair. These cases can be managed with a proximal diverting colostomy alone without suturing of the perforation [3–5].
- Herein, we describe a case of diagnostic laparoscopy and laparoscopic diverting sigmoid loop colostomy for an extraperitoneal rectal injury that was too high for a transanal approach.
INTRODUCTION
- A 41-year-old male was transferred to the emergency room from another hospital after sustaining a penetrating injury caused by a tree limb. On arrival, he was alert, with blood pressure 120/80 mmHg, pulse rate 80/min, respiratory rate 20/min, and body temperature, 36.8°C. He had no significant medical history. Physical examination revealed a small entrance wound with a small amount of visible bleeding on the medial left upper thigh, and a perianal bruise (Fig. 1). Digital rectal examination was unremarkable. Hemoglobin was 13.4 g/dL, with no active bleeding focus. No transfusion was required.
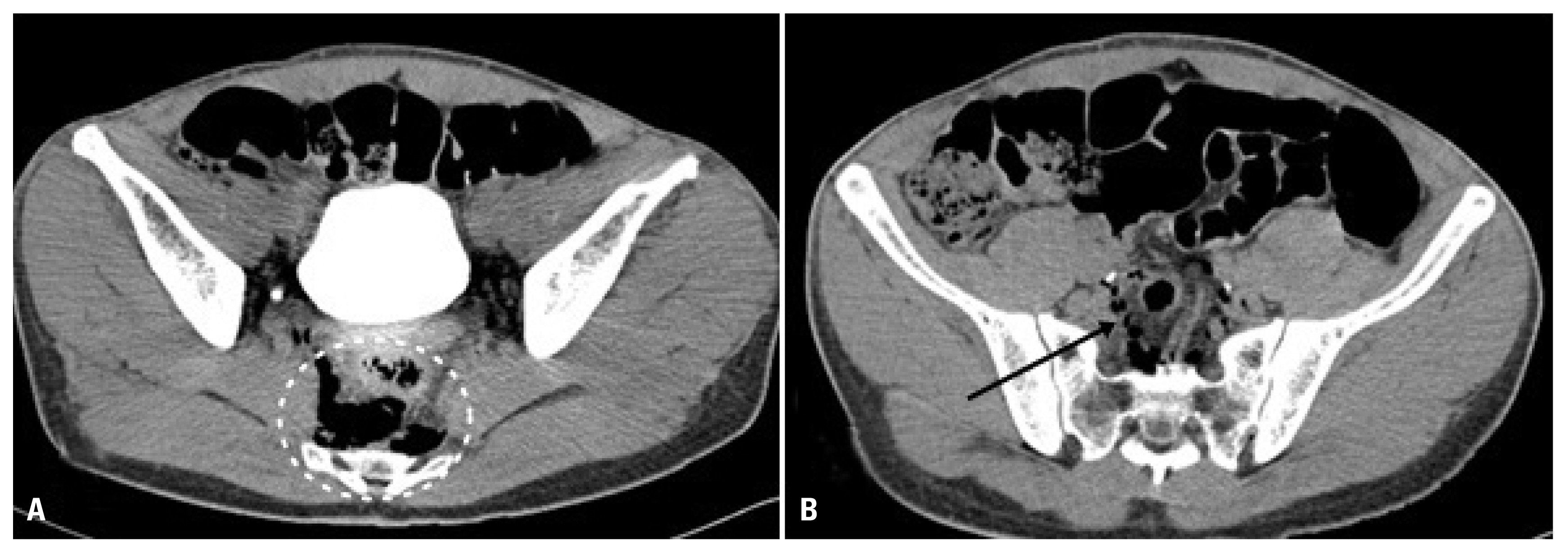
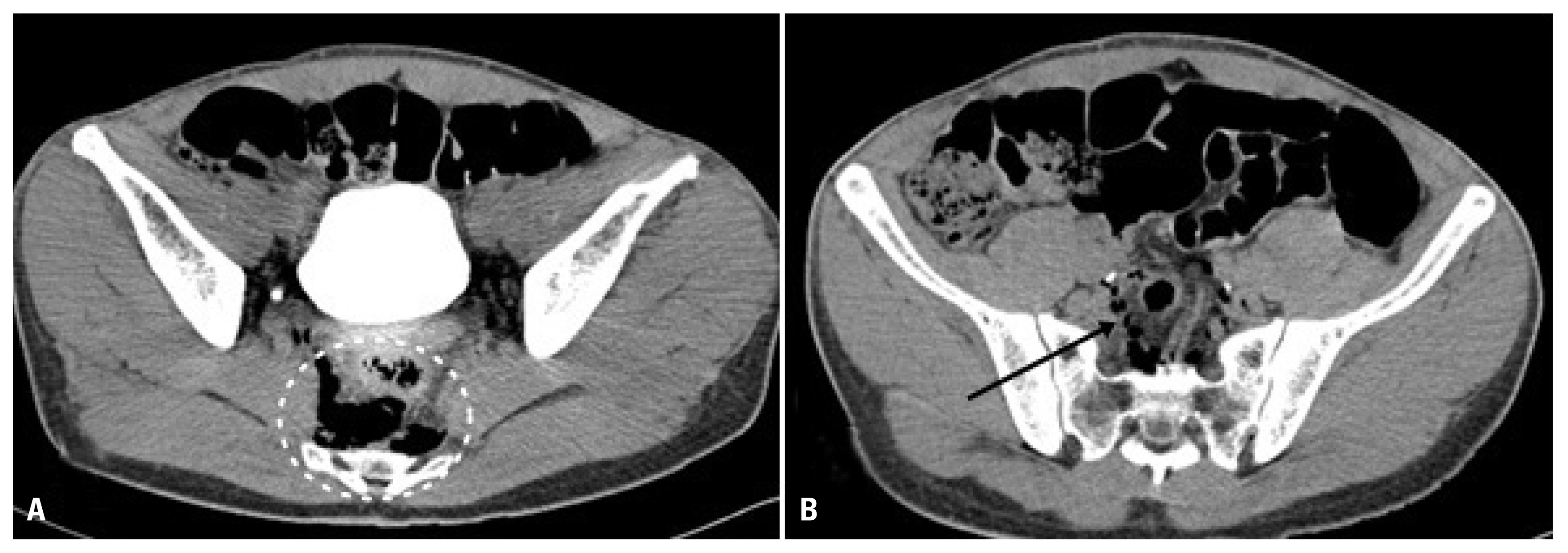
- Abdominal computed tomography (CT) revealed significant air density in the perirectal space and retroperitoneum, implying rectal perforation (Fig. 2). Because there was no extraluminal air density in the abdomen on CT, we presumed no intraperitoneal rectal perforation. The extraperitoneal rectal perforation was identified preoperatively by sigmoidoscopy. In sigmoidoscopy, ulcerative lesion with blood clots suspicious of perforation was found in mid rectum.
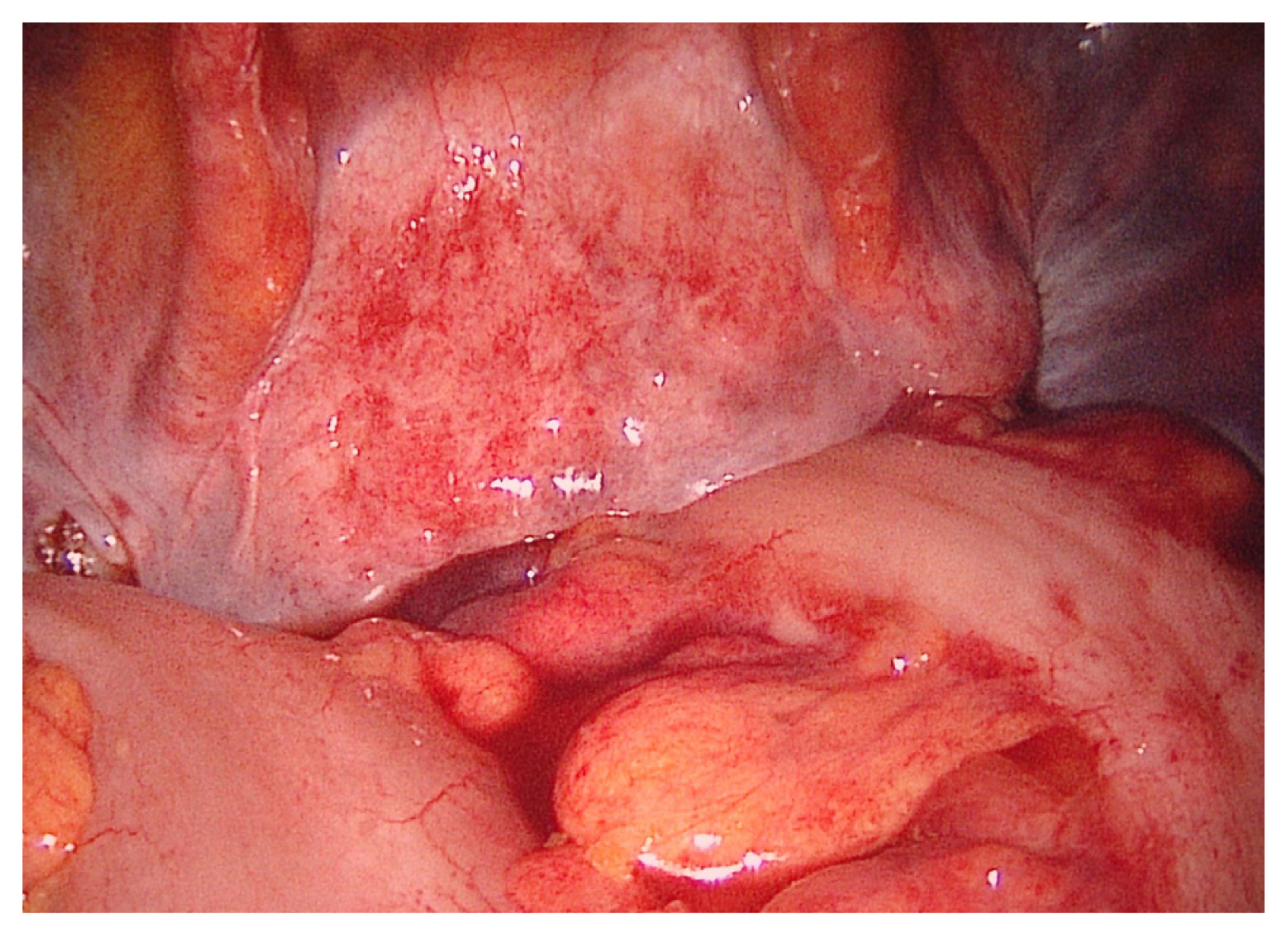
- We performed emergency surgery for diagnosis and treatment. Diagnostic laparoscopy was performed to rule out an intraperitoneal rectal perforation. Findings included petechial hemorrhages and a small hemoperitoneum (Fig. 3), but perforation was not detected. Liver cirrhosis was incidentally detected. As there was no intraperitoneal perforation, we decided to perform diverting sigmoid loop colostomy rather than transanal repair of the rectal injury. After dissection between the sigmoid colon and tissues near the colon to enable lifting to the anterior wall for the colostomy, a Jackson-Pratt drain was inserted into the pelvis for fluid drainage. After gas exsufflation, we successfully completed the loop colostomy (Fig. 4). The total operative time was 75 minutes. The patient was discharged on postoperative day 5 without any complications. Colostomy closure was successfully performed on day 75 following the original operation.
CASE REPORT
- Because of its unique advantages, laparoscopy has been popular for management of various surgical situations. Likewise, in trauma field, laparoscopic use including the diagnostic laparoscopy has been expanded. However, limitations and contraindications cause some clinicians to perform immediate laparotomy, because of concern about hemodynamic instability, diffuse peritonitis, or evisceration [2,6]. Therefore, it is important to define relevant indications. Our patient was hemodynamically stable, and had no other contraindication for diagnostic laparoscopy. Some authors expressed concern that diagnostic laparoscopy performed by a surgeon with limited experience would result in missed injuries [7]. However, preoperative CT helps the surgeon to plan an operation and know which organ is damaged. Based on preoperative CT, we presumed no intraperitoneal organ injuries, and diagnostic laparoscopy avoided unnecessary laparotomy. Additionally, we incidentally diagnosed liver cirrhosis, and the patient was treated postoperatively.
- Rectal injuries have different treatment options, depending on anatomical location and severity of injuries. Because of anatomical and clinical similarity, the vast majority of intraperitoneal rectal injuries are managed by primary repair [8]. The classic management of penetrating extraperitoneal rectal injuries include proximal fecal diversion, presacral drainage, and distal rectal washout. For patients with nondestructive extraperitoneal rectal injuries, an Eastern Association for the Surgery of Trauma practice management guideline conditionally recommends against the routine use of presacral drains and distal rectal washout. Even if proximal diversion maybe somewhat advocated, the role of routine use has been challenged [3]. However, some extraperitoneal injuries like our case are difficult to repair because their anatomical location is too low for a transabdominal approach and too high for a transanal approach. These cases can be managed safely with a proximal diverting colostomy alone, without repair of the perforation [3–5]. Therefore, we performed diverting sigmoid loop colostomy only without looking for the perforation site. Previous evidence reported the usefulness of diagnostic laparoscopy and laparoscopic diverting loop sigmoid colostomy in low-velocity gunshot injuries with extraperitoneal rectal injuries [4,5]. However, in South Korea, in terms of the law, the occurrence of the gunshot injuries is extremely rare. We presumed that the mechanism of injuries in low-velocity penetrating trauma would be similar and successfully used the same approach. Even though liver cirrhosis might affect recovery, the patient was discharged on postoperative day 5 without any complications.
- The appropriate use of laparoscopy is associated with better patient outcomes. However, considerable laparoscopic experience is needed for effective use [7]. The government of South Korea prohibits the non-traumatic emergency general surgery done by trauma surgeons in regional trauma centers which receive the financial support by the government, and they had relatively fewer opportunities for laparoscopic experience. Nonetheless, diagnostic laparoscopy, especially with preoperative CT, and laparoscopic diverting sigmoid loop colostomy do not need complicated techniques. The operative time for our case was 75 minutes, making it feasible even for the surgeon without extensive laparoscopy experience, and was comparable to that reported in another study [9].
- The optimal timing of colostomy closure is unclear. A minimum of 3 months has been advocated traditionally, but subsequent studies showed the closure earlier than 3 months is safe. Recent studies even recommended closure during the initial hospitalization, sometimes within 2 weeks from the original operation [10–13].
- Extraperitoneal rectal perforation may be hard to repair primarily. However, diagnostic laparoscopy and laparoscopic diverting sigmoid loop colostomy in this clinical situation can be a feasible treatment option for trauma surgeons.
DISCUSSION

Fig. 2Abdominal computed tomography showing air density in the perirectal space (A, white circle) and retroperitoneum (B, black arrow).

- 1. Sauerland S, Agresta F, Bergamaschi R, Borzellino G, Budzynski A, Champault G, et al. Laparoscopy for abdominal emergencies: evidence-based guidelines of the European Association for Endoscopic Surgery. Surg Endosc 2006;20:14–29.ArticlePubMedPDF
- 2. Zantut LF, Ivatury RR, Smith RS, Kawahara NT, Porter JM, Fry WR, et al. Diagnostic and therapeutic laparoscopy for penetrating abdominal trauma: a multicenter experience. J Trauma 1997;42:825–9; discussion 829–31, ArticlePubMed
- 3. Velmahos GC, Gomez H, Falabella A, Demetriades D. Operative management of civilian rectal gunshot wounds: simpler is better. World J Surg 2000;24:114–8.ArticlePubMedPDF
- 4. Navsaria PH, Shaw JM, Zellweger R, Nicol AJ, Kahn D. Diagnostic laparoscopy and diverting sigmoid loop colostomy in the management of civilian extraperitoneal rectal gunshot injuries. Br J Surg 2004;91:460–4.ArticlePubMed
- 5. Navsaria PH, Graham R, Nicol A. A new approach to extraperitoneal rectal injuries: laparoscopy and diverting loop sigmoid colostomy. J Trauma 2001;51:532–5.ArticlePubMed
- 6. Sosa JL, Arrillaga A, Puente I, Sleeman D, Ginzburg E, Martin L. Laparoscopy in 121 consecutive patients with abdominal gunshot wounds. J Trauma 1995;39:501–4; discussion 504–6, ArticlePubMed
- 7. Zafar SN, Onwugbufor MT, Hughes K, Greene WR, Cornwell EE 3rd, Fullum TM, et al. Laparoscopic surgery for trauma: the realm of therapeutic management. Am J Surg 2015;209:627–32.ArticlePubMed
- 8. Mattox KL, Moore EE, Feliciano DV. Trauma. 7th ed. New York: McGraw Hill; 2013.
- 9. Trejo-Ávila ME, Valenzuela-Salazar C, Betancourt-Ferreyra J, Fernández-Enríquez E, Romero-Loera S, Moreno-Portillo M. Laparoscopic versus open surgery for abdominal trauma: a case-matched study. J Laparoendosc Adv Surg Tech A 2017;27:383–7.ArticlePubMed
- 10. Parks SE, Hastings PR. Complications of colostomy closure. Am J Surg 1985;149:672–5.ArticlePubMed
- 11. Renz BM, Feliciano DV, Sherman R. Same admission colostomy closure (SACC). A new approach to rectal wounds: a prospective study. Ann Surg 1993;218:279–92; discussion 292–3, ArticlePubMedPMC
- 12. Khalid MS, Moeen S, Khan AW, Arshad R, Khan AF. Same admission colostomy closure: a prospective, randomised study in selected patient groups. Surgeon 2005;3:11–4.ArticlePubMed
- 13. Velmahos GC, Degiannis E, Wells M, Souter I, Saadia R. Early closure of colostomies in trauma patients--a prospective randomized trial. Surgery 1995;118:815–20.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- The floating rectum
Sean Ng Kwet Chi Ng Ying Kin, William Jiang, Asiri Arachchi, Hanumant Chouhan
ANZ Journal of Surgery.2022; 92(1-2): 264. CrossRef
 PubReader
PubReader ePub Link
ePub Link Cite
Cite